Experiments confirm anti-biotic properties of birch bark extract
The bark of birch trees has been used to produce tar for more than 150 000 years. The centre photo shows birch bark tar condensed onto a rock that borders a hearth. When scraped off the rocks, the viscous tar can be used as both an adhesive and antibiotic.
Neanderthals probably used birch tar for multiple functions, including treating their wounds, according to a study published March 18, 2026 in the open-access journal PLOS One by a team of researchers led by Tjaark Siemssen of the University of Cologne, Germany, and the University of Oxford, UK.
Birch tar is commonly found at Neanderthal archaeological sites, and in some cases this tar is known to have been used as an adhesive to assemble tools. Recently, some researchers have raised the question of whether Neanderthals had multiple uses for this substance. For instance, Indigenous communities in northern Europe and Canada use birch tar to treat wounds, and there is growing evidence that Neanderthals also employed a variety of medical practices.
To investigate the medicinal potential of birch tar, Siemssen and colleagues extracted tar from modern birch tree bark, specifically targeting species known from Neanderthal sites. They used multiple extraction methods, including distillation of tar in a clay pit and condensation of tar against a stone surface, both of which would have been methods available to Neanderthals. When exposed to different strains of bacteria, all of the tar samples were found to be effective at hindering the growth of Staphylococcus bacteria known to cause wound infections.
These experiments not only support the efficacy of Indigenous medicinal practices, but also reinforce the possibility that Neanderthals used birch tar to treat wounds. The authors note that there are other potential uses of birch tar, such as insect repellent, as well as other plants to which Neanderthals had access. Further exploration of the multiple potential uses of these natural ingredients will enable a more thorough understanding of Neanderthal culture.
The authors add: “We found that the birch tar produced by Neanderthals and early humans had antibacterial properties. This has important implications for how Neanderthals may have mitigated disease burden during the last Ice Ages, and adds to a growing set of evidence on healthcare in these early human communities.”
“By bringing together research on indigenous pharmacology and experimental archaeology, we begin to understand the medicinal practices of our distant human ancestors and their closest cousins. Additionally, this study of ‘palaeopharmacology’ can contribute to the rediscovery of antibiotic remedies whilst we face an ever more pressing antimicrobial resistance crisis.”
“The messiness of birch tar production deserves a special mention. Every step of the production is a sensory experience in itself, and getting the tar off our hands after spending hours at the fire has been a challenge every time.”
Image caption: The bark of birch trees has been used to produce tar for more than 150,000 years. The centre photo shows birch bark tar condensed onto a rock that borders a hearth. When scraped off the rocks, the viscous tar can be used as both an adhesive and antibiotic.
Citation: Siemssen T, Oludare A, Schemmel M, Puschmann J, Bierenstiel M (2026) Antibacterial properties of experimentally produced birch tar and its medicinal affordances in the Pleistocene. PLoS One 21(3): e0343618. https://doi.org/10.1371/journal.pone.0343618
Author countries: U.K., Canada, Belgium, Germany
Funding: Tjaark Siemssen is funded by the Boise Trust of the University of Oxford and the German Academic Scholarship Foundation (Studienstiftung). Aderonke Oludare was funded by Canadian Institutes of Health Research (CIHR) Project Grant 420598 awarded to Matthias Bierenstiel. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests: The authors have declared that no competing interests exist.
A new study has found that metformin may mimic one of exercise’s core biological effects in men with prostate cancer, raising levels of a molecule tied to energy balance and weight control even when patients are inactive. The findings suggest that metformin could help counter the metabolic strain of hormone therapy, when fatigue and other side effects often limit physical activity.
Led by physician-scientists at Sylvester Comprehensive Cancer Center, part of the University of Miami Miller School of Medicine, the study appears in the journal EMBO Molecular Medicine.
Exercise is one of the most reliable ways to support health during cancer treatment. It helps regulate weight, blood sugar, and cardiovascular health – factors that shape how patients feel during therapy and how well they recover afterward.
For many people with cancer, however, regular exercise isn’t always feasible. Fatigue, hormone therapy, pain, or advanced disease can limit physical activity precisely when metabolic health becomes most important.
That reality has led researchers to ask a practical question: If exercise confers its benefits through specific biological signals, could some of those signals be activated in other ways?
According to the research, the answer may be yes. Sylvester investigators report that metformin raises levels of a naturally occurring molecule involved in how the body manages energy and weight in prostate cancer patients.
The finding does not suggest that a pill can replace physical activity. Instead, it offers insight into the internal pathways that underlie exercise’s metabolic benefits – and how those pathways might still be engaged when movement is limited.
“This study reflects what’s possible when laboratory science, metabolic biology, and clinical investigation are intentionally brought together for transdisciplinary studies,” said Sylvester researcher and first author, Marijo Bilusic, MD, PhD, genitourinary medical oncologist and professor of medicine and medical oncology at the Miller School. “The result isn’t a new cancer biomarker, but a clearer understanding of how a widely used drug may support metabolic health during prostate cancer treatment – an outcome that matters to patients and clinicians alike.”
The molecule at the heart of the study
At the center of the collaborative, team-science study is a molecule called N-lactoyl-phenylalanine (Lac-Phe). While its name is technical, its role is relatively simple.
Lac‑Phe is produced when the body is under metabolic demand. It forms when lactate, which accumulates during exertion, combines with phenylalanine, a basic building block of protein. Scientists first took notice of Lac‑Phe because its levels spike after intense exercise, coinciding with shifts in energy use and appetite regulation.
In preclinical and early human studies, higher Lac‑Phe levels have been associated with reduced appetite and improved weight control – two effects commonly linked to regular physical activity.
Lac-Phe does not rise only with exercise. Scientists observed elevated Lac-Phe levels in people taking metformin, even in the absence of physical activity. That overlap raised an important question for cancer care: Could a pathway typically associated with exercise be activated pharmacologically in patients whose treatments limit movement?
Why prostate cancer patients are a focus
To explore that question, the Sylvester team focused on prostate cancer, where hormone-based therapies are known to disrupt metabolism, contributing to weight gain, insulin resistance, and cardiovascular risk.
Notably, Lac-Phe levels in patients treated with metformin approximated those previously reported after strenuous exercise. This occurred even though patients were not exercising at the time of blood collection, and the effect persisted after hormone therapy began.
“From a clinical standpoint, seeing a metabolic signal that mirrors what we associate with intense exercise was striking,” said Bilusic. “For patients whose treatments or symptoms limit physical activity, that kind of effect could be especially meaningful.”
Higher Lac-Phe levels were not associated with anti-tumour response to metformin. The metabolite did not correlate with changes in prostate-specific antigen (PSA), a standard marker used to monitor prostate cancer.
What Lac-Phe might mean for patients
That distinction is central to the study’s interpretation. While more expanded studies are needed to determine the utility of Lac-Phe as a marker of anticancer efficacy, it appears to reflect how the body manages energy, weight and metabolic strain during treatment. These results were confirmed to ensure the findings were not limited to one clinical setting. In fact, increases were also observed in patients receiving other metabolic therapies, suggesting Lac-Phe may reflect a broader metabolic response rather than a drug‑specific effect.
“Cancer therapy often affects the body in ways that go beyond the tumour,” said Sylvester researcher Priyamvada Rai, PhD, co-leader, Tumor Biology Program and professor of radiation oncology at the Miller School. “Supporting metabolic health can influence how patients tolerate treatment and how they feel over time, even if it doesn’t directly change tumour growth. This study was an opportunity to investigate molecular pathways that can be therapeutically activated for better outcomes to treatments that induce metabolic stress.”
Metformin raises a stress hormone called GDF‑15, but this study found that Lac‑Phe was more closely tied to weight changes. Because the two didn’t rise together, metformin likely affects weight through multiple pathways, with Lac‑Phe playing a bigger role.
Taken together, the findings offer a clearer picture of how a widely used diabetes medication may influence metabolic health during prostate cancer care.
“What’s encouraging about this work is that it reminds us cancer care isn’t only about targeting tumours – it’s also about supporting the whole patient,” said Rai. “By better understanding how treatments affect metabolism, we can begin to identify ways to help patients maintain strength, resilience, and quality of life throughout their care.”
Despite South Africa’s laws and policies, access to healthcare remains an issue, particularly for non-citizens. Photo by Hush Naidoo on Unsplash
By Teri Brown and Thembi Mahlathi
The media has reported several incidents where people were turned away at public healthcare facilities because they did not possess South African identity documents. As related cases slowly grind through the courts, Teri Brown and Thembi Mahlathi of SECTION27 connect the dots between what the law says and what people are experiencing.
Over the years, many migrants and undocumented people have reached out to SECTION27, where we both work, for assistance. These were often pregnant women, lactating mothers and children under six years, who were denied access to healthcare facilities.
Initially, it was easy to simply write a letter to hospital and clinic personnel where our clients were being denied access. But as time went on, the situation got significantly worse and more migrants were being denied access to public healthcare facilities. Writing letters and asking for meetings clearly wasn’t enough anymore.
We went to court and in April 2023 got an order in which the South Gauteng High Court held that important sections of the National Health Act applies to all pregnant women, lactating women and children under the age of six years, irrespective of their documentation status. This affirmed that in South Africa, they have the right to access free healthcare services at all public health establishments, including hospitals and clinics.
Public sector hospitals and clinics are required to assess the status of migrants and then apply a lawful means test to determine the healthcare services that can be offered to them. However, this does not appear to be done routinely. Instead, particular focus is often placed on South African identity documents, while other forms of documentation held by migrants are disregarded.
There have been incidents where entry to facilities such as Rahima Moosa Mother and Child Hospital in Coronationville and South Rand Hospital in Rosettenville and several clinics across Gauteng have been denied to people, including South African nationals who have the necessary documentation.
Furthermore, we are aware that to avoid being refused healthcare and to demonstrate the urgency of their need for treatment for themselves or their kids, migrants have sometimes been forced to disclose their HIV status – information which they would otherwise have kept private.
In mid-2025, we started receiving a surge of calls from clients complaining about not being able to enter public sector clinics that they were previously assisted at. They informed us that a group of people stationed outside these clinics requested their identity documents, and when they produced their documents confirming either their refugee status or asylum seeker status, they were unlawfully prevented from entering the clinics. These group of people explicitly told them that they should go to a private clinic for treatment or go back to their home country.
Thus, two years after the April 2023 court order, the denial of access to healthcare had worsened, as it was not only women and children who could not access clinics, but anyone who could not provide South African identity documentation. The situation was also exacerbated by the fact that it wasn’t just healthcare staff denying access anymore, but vigilante groups stationed outside healthcare facilities.
Despite the crisis being widely reported, the state failed to address it effectively. We had no choice but to go back to court, and again the court found in our favour.
In December 2025, the South Gauteng High Court ordered the state to take immediate and decisive action to end the obstruction of access to public healthcare facilities in Gauteng. The case was brought by the civil society organisations the Treatment Action Campaign, Doctors Without Borders, and Kopanang Africa Against Xenophobia (the applicants), all represented by SECTION27.
In this landmark judgment, Judge Stuart Wilson concluded that the state entities tasked with upholding the constitutional mandate to safeguard everyone’s right to access healthcare had failed to prevent the obstruction of access to public health facilities. Consequently, this failure was in violation of the constitutional rights of patients seeking care at the Yeoville and Rosettenville clinics.
Despite this court order, our monitoring found ongoing vigilante activity at the two clinics. The applicants then launched an urgent contempt application, heard in March 2026, arguing that the state had failed to fully comply with Judge Wilson’s court order.
Following this, a court ordered settlement agreement was reached with the Gauteng Department of Health and other respondents. Among other things, it required the authorities to take reasonable steps to ensure safe and unhindered access to the Yeoville and Rosettenville clinics, and to report on the implementation by 18 May 2026. It also makes provision to continue legal proceedings if necessary to enforce full compliance with Judge Wilson’s order.
The laws governing healthcare for migrants in South Africa
Taking a step back from this case, and its specific set of facts, it is worth remembering that South African law really does provide extensive protection to migrants who need to access healthcare services.
The right to access healthcare services is guaranteed by section 27 of our Constitution, which states that everyone has the right to have access to healthcare services, and that no one may be refused emergency medical treatment. The term “everyone” is not restricted to South Africans only. It includes everyone within the borders of South Africa, regardless of their nationality.
This right extends to all children living in South Africa under section 28(1)(c) of the Constitution. This guarantees all children access to basic healthcare services dependent on the availability of resources, to which they can never be completely denied.
After the Constitution, the most important piece of healthcare legislation relevant to migrants is the National Health Act (NHA). The NHA assists in giving effect to the constitutional right to basic healthcare services by outlining who can receive services at public clinics free of charge. It obligates the provision of free healthcare services to women who are pregnant or breastfeeding, or children under six. Moreover, the NHA requires that free primary healthcare be provided to those without medical aid. It also makes it clear that those working in healthcare cannot refuse any person emergency medical treatment.
Along similar lines, South Africa’s Refugees Act states that a refugee is entitled to full legal protection, which includes the rights set out in the Bill of Rights, except those reserved for citizens. The Act formally acknowledges that refugees are entitled to the same basic healthcare services and primary education that South African citizens receive. While the Act does not expressly cover undocumented migrants, it is grounded on the principle of non-discrimination, which supports equal access to essential services.
The denial of healthcare services has significant impacts on many aspects of people’s lives. Migrants often become so desperate to receive care that they feel compelled to disclose their HIV status, which infringes on their rights, particularly the constitutional rights to privacy and dignity. It also creates feelings of stigma and discrimination, further marginalising people who are often already vulnerable.
There are also direct health consequences. Denying treatment to a migrant not only negatively impacts that person’s health it can also result in the continued transmission of infectious diseases to both other migrants and South Africans. For example, HIV and TB typically become non-infectious a while after someone starts treatment. Deciding not to treat someone ends up harming everyone. As untreated conditions worsen, it may require emergency medical attention that could have been avoided through early treatment. All of this places extra pressure on an already fragile health system – extra pressure that could be avoided by providing more migrants with healthcare services as soon as they need it.
The failure to provide healthcare services also affects migrants’ livelihoods and well-being. For those who run their own businesses, being unable to access treatment may prevent them from working altogether and could lead to them and other people, possibly South Africans, losing their jobs. Ultimately, this has a ripple effect on the country’s economy, job security, and perpetuates cycles of poverty and vulnerability.
At its heart then, this issue is about who we choose to be as a society. Turning people away at their most vulnerable moments erodes not only their dignity, but also their humanity and ours. In a country built on the values of equality and dignity, we cannot allow this attack on our basic humanity and decency to succeed. We are, and must be, better than that.
*Brown is a legal researcher and Mahlathi is a paralegal with SECTION27. In the court case discussed in this article, SECTION27 represented the Treatment Action Campaign, Médecins Sans Frontiers, and Kopanang Africa Against Xenophobia.
Note: Spotlight is published by SECTION27, but is editorially independent – an independence that the editors guard jealously. Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.
Republished from Spotlight under a Creative Commons licence.
A new study from the University of Minnesota Medical School demonstrated that faecal microbiota transplantation (FMT) can rapidly reverse systemic inflammation and improve survival in patients with fulminant Clostridioides difficile (C. difficile) infection – a life-threatening condition characterised by a sepsis-like state. The findings were published in Clinical Gastroenterology and Hepatology.
C. difficile infection is the most common cause of healthcare-acquired diarrhoeal illnesses. Most of the mortality, estimated at 15 000 people annually in the United States alone, is associated with the severe and fulminant forms of the disease. C. difficile is listed as one of the most urgent infectious disease threats by the Centers for Disease Control and Prevention. The infection occurs in people with disrupted microbial communities in the gut, most commonly by antibiotic medications.
In this study, investigators implemented a standardised FMT protocol developed at the University of Minnesota specifically for critically ill patients who were deteriorating despite intensive antibiotic therapies and were often too unstable for surgery. Among 18 patients treated, FMT was associated with rapid declines in inflammatory markers and achieved a 78% 30-day survival.
“There is an important caveat to our findings – the window for the FMT intervention is very narrow because these patients are generally extremely sick,” said Alexander Khoruts, MD, professor at the University of Minnesota Medical School, director of the UMN Microbiota Therapeutics Program and a gastroenterologist with M Health Fairview. “Therefore, the FMT formulation needs to be easily accessible. We are in a unique position at the University because we have a facility in our institution where our FMT products are manufactured in accordance with pharmaceutical standards, and treatment units are always on hand in our cryobank.”
The University of Minnesota Microbiota Therapeutics program is the leading program in the world in developing microbiome-targeted therapies with live microbial communities. As a result of the team’s work, M Health Fairview recently implemented a dedicated system that alerts providers to hospitalized patients at risk of developing severe C. difficile infection so that they can get access to the optimal treatments earlier.
Importantly, the findings also suggest an entirely novel mechanism by which FMT can modulate systemic inflammation in severe C. difficile infection. This is a topic of ongoing research. The team is also currently working to make this FMT treatment option more widely available to patients across the United States.
Researchers discovered perfluorodecanoic acid is the most toxic during foetal craniofacial development
Credit: Chemical Research in Toxicology (2026). doi:10.1021/acs.chemrestox.5c00468
Researchers have long associated per- and polyfluoroalkyl substances (PFAS), commonly known as “forever chemicals,” to certain severe birth defects but exactly how these pollutants harm a developing foetus has remained mostly a mystery. New research now provides the first clear molecular explanation, showing how one PFAS, called perfluorodecanoic acid (PFDA), can trigger craniofacial abnormalities before birth.
“Most people are exposed to small amounts of PFAS in everyday life but higher exposure can occur through contaminated water, living near manufacturing sites or certain jobs like firefighting and ski waxing, which is why it’s so important to understand the chemicals better,” said the paper’s senior author Jed Lampe, PhD, associate professor at University of Colorado Anschutz Skaggs School of Pharmacy and Pharmaceutical Sciences. “We wanted to understand which PFAS compounds are truly harmful during foetus development, especially for people with higher exposure, and how they cause damage.”
There are approximately 15 000 PFAS used in consumer and industrial products but scientists are increasingly finding that only some pose serious health risks. In this study, Lampe worked with the paper’s first author Michaela Hvizdak and co-author Sylvie Kandel to test 13 commonly found PFAS and discovered PFDA as the most toxic during foetal craniofacial development.
They demonstrated a possible link between PFDA and the extensive facial changes observed in humans and laboratory animals, with some estimates indicating a 10% increased risk at extremely low exposure levels.
“This finding moves us beyond association by providing a clear explanation for how PFDA can interfere with foetal development. It’s a critical step toward understanding a vast and complex class of environmental chemicals,” said Lampe.
The cause of underdeveloped eyes and an abnormal jaw
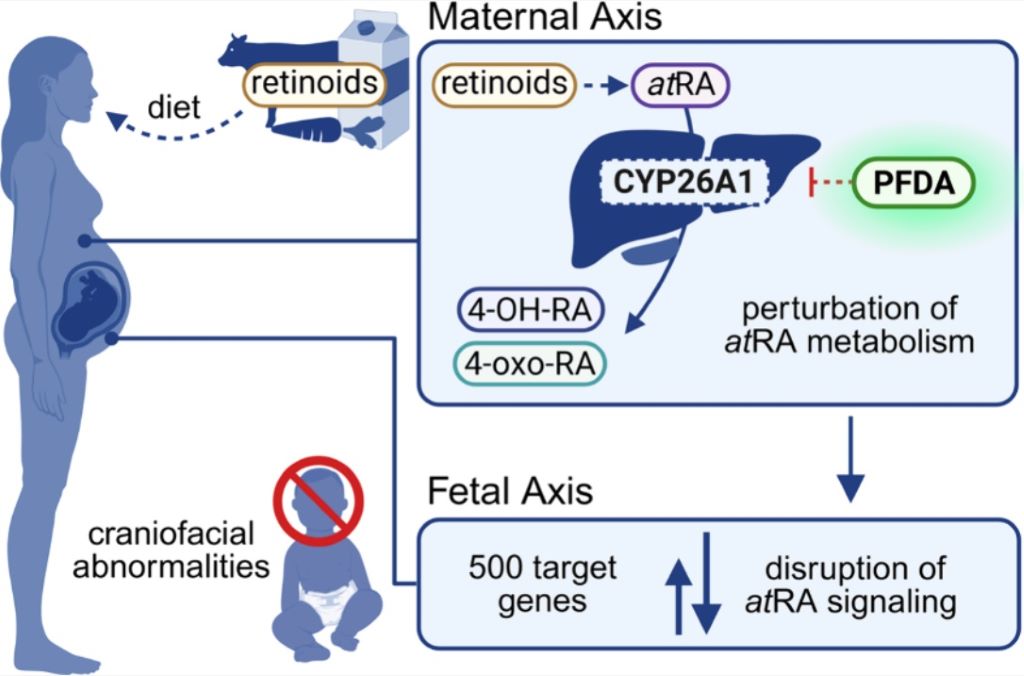
They found that PFAS disrupts retinoic acid, a molecule essential for shaping the face and head during early pregnancy. Retinoic acid regulates hundreds of genes and its levels must be controlled. Because a foetus cannot produce or safely eliminate excess retinoic acid, it relies entirely on the mother to maintain the homeostatic balance of the hormone.
The researchers discovered PFDA blocks CYP26A1, a key enzyme responsible for breaking down excess retinoic acid. When this enzyme is inhibited, retinoic acid levels can rise too high, disrupting normal facial development. PFDA also suppresses the genes that produce this enzyme through a separate biological pathway, delivering a “double hit” to the system that regulates early development.
“As a result, severe craniofacial abnormalities can develop, including underdeveloped eyes and abnormal jaw formation, which were the most common effects of PFDA exposure during foetal development,” said Lampe.
The researchers hope by providing a molecular explanation for this abnormality that the research and scientific community can work to develop targeted laboratory assays and computer‑based screening tools to quickly rank PFAS by risk. They say this could help regulators and manufacturers distinguish more dangerous compounds from safer alternatives and guide the design of less toxic chemicals in the future.
They also hope the research can open the door to practical interventions for people with higher exposure, such as firefighters and ski wax technicians. This could include looking into how to reduce exposure levels and whether strategies can be developed to lower PFDA during pregnancy to protect foetal development.