Prenatal magnesium sulfate and steroids can reduce the risks of cerebral palsy and respiratory complications in preterm infants. A review in the International Journal of Gynecology & Obstetrics found that despite being recommended internationally for pregnant women at risk of preterm delivery, these medications are used variably between and within countries.
When they analysed 2012–2024 information on 45 619 babies born at 24–32 weeks’ gestation at 1111 hospitals in an international network, along with information from the UK National Neonatal Research Database and a literature review, investigators found that on average, less than half of infants had been exposed to preterm magnesium sulfate in middle-income countries, and approximately three-quarters in high-income countries. Even within high-income countries, there were large discrepancies in care. Preterm steroids were used more frequently with less variation, although treatment gaps were still apparent.
“Our study has highlighted the international disparities in how two key treatments to protect pre-term babies are implemented. These gaps aren’t because of a lack of evidence,” said corresponding author Hannah B. Edwards, MA, MSc, of the University of Bristol, in the UK. “Lessons can be learned from successful implementation programs like PReCePT, which has transformed use of magnesium sulphate in pre-term births in England. The bigger-picture goal should now be to ensure that no matter where a baby is born, their mother has access to the evidence-based treatments that offer the best start in life.”
We’ve known for a long time that women are more likely than men to have migraine attacks.
As children, girls and boys experience migraine equally. But after puberty, women are two to three times more likely to experience this potentially debilitating condition.
Recently, an Australian study showed it may be even more common than we previously thought – as many as one in three women live with migraine.
For comparison, migraine affects roughly one in 15 men in Australia.
So, what’s behind the difference? Here’s what we know.
More than a headache
Migraine is not just a bad headache – it is a complex disorder that causes the brain to process sensory information abnormally.
This means “migraine brains” can have difficulty processing information from any of the five senses:
sight (leading to problems with light sensitivity and glare)
sound (leading to noise sensitivity)
smell (certain smells can trigger headaches)
touch (leading to face or scalp tenderness)
taste (causing distorted taste, nausea and vomiting).
Migraine attacks typically last anywhere from four hours to three days – but can be longer.
In addition to the symptoms above, attacks can include throbbing head pain, dizziness, fatigue and difficulty concentrating. It is these extra symptoms that help diagnose migraine – not the location of head pain or pain severity.
Why are attacks more frequent in women?
Puberty is when the difference between men and women emerges. This is when our bodies massively increase the production of sex hormones.
People are often surprised to learn that both men and women produce oestrogen, progesterone and testosterone. Testosterone levels are higher in men, whereas women have higher levels of oestrogen and progesterone.
However, it is not just the type of hormone that makes a difference, but the way they fluctuate over time.
For many women, there are certain “milestone moments” when their migraine tends to worsen due to hormonal fluctuations – puberty, menstruation, pregnancy and perimenopause (the lead-up to your final period).
For example, some women notice migraine flare-ups every month, linked to phases in their monthly menstrual cycle when oestrogen levels drop.
They might even be able to predict when their period will start, as migraine attacks typically start a few days before the bleeding.
How hormones affect the brain
Women with migraine can be more sensitive to hormonal changes. This is particularly the case for sudden decreases in oestrogen. But even more subtle changes to hormone levels can cause migraine attacks.
These hormonal changes can activate brain processes that trigger migraine, such as cortical spreading depression. This is a very slow wave of electrical activity that spreads in the brain, causing some areas to function more slowly than others after it passes.
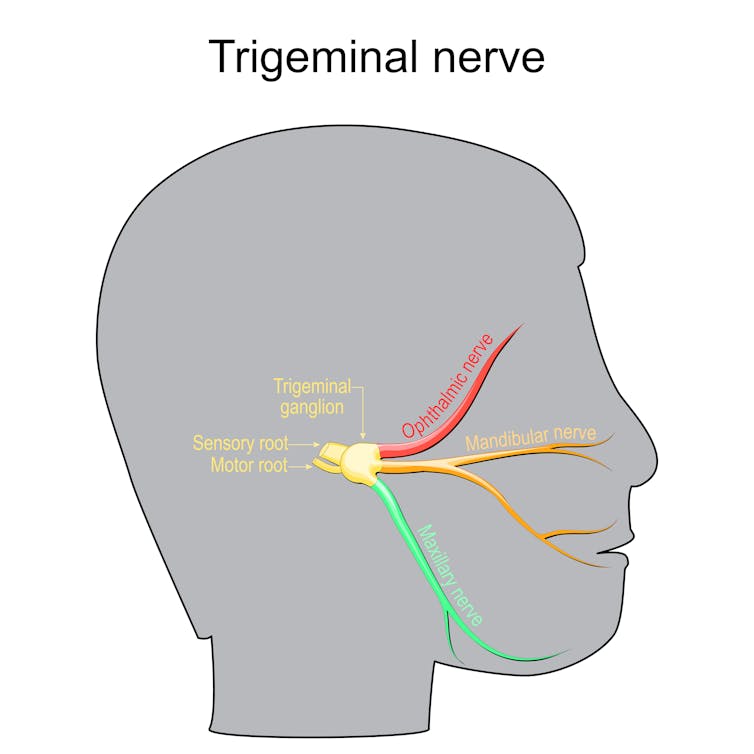
Decrease in oestrogen can also affect how we receive and process information through the trigeminal nerve. This plays a key role in the onset and maintenance of migraine pain.
Oestrogen can affect how we process information through the trigeminal nerve. ttsz/Getty
All kinds of fluctuations can be a trigger
Pregnancy can often destabilise migraine again and make attacks more likely, even when someone has previously enjoyed a period of good migraine control.
Migraine symptoms often become uncontrolled in the first trimester in particular, due to rapid hormonal changes needed to sustain a pregnancy. This usually settles in the second and third trimesters, when hormonal changes stabilise.
However, giving birth is yet another change.
Towards the end of pregnancy, oestrogen levels can be 30 times higher than pre-pregnancy levels, and progesterone can be 20 times higher. When these hormones plummet back to normal after giving birth, migraine attacks can often sharply worsen again.
Perimenopause can also involve random surges of oestrogen from the dwindling supplies of eggs within the ovaries – which previously produced these hormones cyclically and in abundance. This irregular hormone production can cause random spikes in migraine attacks. It can be extra challenging when combined with other symptoms of menopause such as hot flushes or mood changes.
Hormonal contraceptives and menopause hormone therapy can also affect migraine control. Sometimes, supplementing hormones at a regular, steady daily dose can help manage the hormone-sensitive headaches and other symptoms. However, for others, adding extra hormones can cause head pain to flare up.
Does migraine run in the family?
Genes also play a role. It’s not a coincidence that migraine is passed down in families through the maternal side.
This is because mothers pass on mitochondria to children (while fathers do not). Mitochondria are parts inside the cell that control energy.
People with migraine have fewer functional enzymes within their mitochondria, meaning their brains are in an energy-deficient state. This worsens with migraine attacks as there is even more stress to the system.
This is also why extra stress (such as sleep deprivation, missed meals, or emotional stress) can trigger a migraine and worsen pain.
There is also a strong link between migraine in women and anxiety and depression – conditions women are more likely to develop in response to stressful life events.
Knowing your own patterns
If you suspect hormones may be affecting your migraine attacks, it is helpful to keep a diary of symptoms, including headaches. Mark each day per month where you get migraine symptoms, as well as your period, to find patterns.
Identifying patterns in pain flares helps doctors guide you to a personalised medication plan, which may include hormone therapies or non-hormonal therapies.
Long-term data suggests an overall cure rate of 42%
Photo by National Cancer Institute on Unsplash
Unlike some other forms of lymphoma, advanced stage follicular lymphoma is considered incurable. But a new analysis of long-term data on patients treated for the disease years ago with standard regimens of immunotherapy and a chemotherapy combination known as CHOP suggests that many of those patients can now be considered cured.
The analysis is just published in the journal JAMA Oncology.
“A subset of advanced-stage follicular lymphoma patients can achieve cure with CHOP-based chemoimmunotherapy, as relapse rates decline over time,” said Wilmot Cancer Institute Director Jonathan W. Friedberg, MD, MMSc, at the University of Rochester Medical Center, who is senior and corresponding author on the paper.
“This finding represents a paradigm shift in our understanding and approach to follicular lymphoma, with broad implications for initial patient discussions and future research strategies.”
Historically, follicular lymphoma has been considered an incurable disease, with most patients experiencing relapses even years after initial treatment.
The JAMA Oncology paper reports on an analysis of follow-up data from patients with advanced follicular lymphoma who had been treated with a standard first-line chemoimmunotherapy regimen on a large clinical trial.
Roughly 70 percent of the patients remained alive 15 years after beginning treatment, and a statistical method known as cure modelling estimated that 42% of treated patients had been cured.
Cure modelling incorporates background mortality rates in an analysis of patient survival data to estimate what fraction of a group of patients can be considered cured of a disease. Such modelling accounts for the fact that over time some patient deaths will occur that are unrelated to the given disease.
The researchers applied a cure model to 15-year follow-up data from the S0016 clinical trial conducted by the SWOG Cancer Research Network, a clinical trials group funded by the National Cancer Institute (NCI), part of the National Institutes of Health (NIH), with the participation of other groups within the NCI-funded National Clinical Trials Network (NCTN).
This phase 3 trial, which opened in 2001, enrolled patients with untreated advanced-stage CD20-positive follicular lymphoma and randomised 531 of them to one of two treatments, both of which were built around a core chemotherapy regimen known as CHOP (cyclophosphamide, hydroxydaunorubicin, vincristine, and prednisone). One arm treated patients with rituximab plus the CHOP combination (R-CHOP), while the other arm used CHOP followed by radioimmunotherapy (CHOP-RIT). Primary results of the S0016 trial were published in 2013 (Press, OW. J Clin Oncol. 2013).
The S0016 modeling, including cure analysis, was carried out by Michael LeBlanc, PhD, a biostatistician at Fred Hutch Cancer Center and director of SWOG’s Statistics and Data Management Center (SDMC), and Hongli Li, MS, also at Fred Hutch and the SWOG SDMC.
It showed that, with a median follow-up time of 15.5 years after a patient had begun treatment, the rate of disease relapse dropped substantially over time, falling from 6.8% of patients relapsing in the first 5 years to only 0.6% relapsing between years 15 and 20.
Fifteen years after starting treatment, about 70%of patients remained alive. The analysis also showed no statistically significant difference between the two treatment arms in the rates of 15-year overall survival.
Based on their work, the authors conclude that a substantial subset of patients with advanced-stage follicular lymphoma can, when treated with a standard regimen that includes immunotherapy and chemotherapy, achieve a functional cure – defined as having no chance of lymphoma recurring during the patient’s expected lifespan.
“These results reinforce that front-line chemoimmunotherapy remains an important option – particularly for appropriate patients – because it can deliver long-term disease control after a time-limited course of treatment, ” said first author Mazyar Shadman, MD, MPH, of Fred Hutch Cancer Center. Shadman is medical director of cellular immunotherapy at Fred Hutch, where he holds the Innovators Network Endowed Chair.
“As we bring novel agents into the first-line setting, the durability seen here sets a high benchmark; new strategies should aim not only to improve short-term response rates but to match or exceed long-term remission and cure potential.”
The idea that many of these patients can be cured could change how newly diagnosed patients are counseled and could eliminate the need for indefinite oncology and radiologic follow-up visits after treatment, with patients eventually transitioning from oncology care back to a primary care team.
A major new study, led by Queen Mary University of London and funded by the National Institute for Health and Care Research (NIHR) has been published in The Lancet Public Health. It found that out of the five million surgical procedures performed each year by the NHS, around 300 000 are carried out on individuals considered high-risk, and within 90 days of surgery, these high-risk patients account for:
four out of five deaths
over half of all hospital bed days
nearly one-third of emergency readmissions
While surgery is safer than ever for most people and remains the best treatment option for many conditions, this study highlights the urgent need to identify high-risk patients earlier, to provide care that is better tailored to their individual needs, and for doctors and patients to have more open, honest conversations about the risks and long-term outcomes for surgery at an individual level.
It also shows that high-risk patients, who tend to be older and live with several long-term health conditions such as heart disease, have poor outcomes not because of technical failings in surgery or anaesthesia, but due to post-operative complications relating to chronic health conditions, age and frailty. Therefore, the findings demonstrate the need for greater investment in specialist perioperative services that focus on the care of older, high-risk patients before, during and after surgery.
Rupert Pearse, Professor and Consultant in Intensive Care Medicine at Queen Mary University of London and Barts Health NHS Trust, and co-lead of the study said: “While surgery is safer than ever before, our findings clearly show that high-risk patients are more likely to have poor outcomes and experience harm after surgery than those deemed low-risk.
“Although these patients make up fewer than one in ten surgical cases, their numbers are increasing as the population ages and more people live longer with chronic illness. It is therefore vital that we work to improve care for this group of patients, pre- and post-surgery, including having open conversations with patients about the individual risk of their procedure.”
He continues: “For many years, surgical success has often been judged by survival at thirty days. Our study shows that this measure does not give the full picture of what happens to many high-risk patients in the months and years after surgery. By looking at longer-term survival and other factors such as time spent in hospital and quality of life, we could make a real difference to patients and potentially help relieve pressure on the wider NHS.”
The study is one of the largest analyses of surgical outcomes ever carried out in the UK. It analysed health records from 13 million adults who had 16.1 million surgical procedures in England, Scotland and Wales between 2015 and 2019.
Mark Bishop, Deputy Chairperson of the Hospital Association of South Africa (HASA) and Chief Commercial Officer at Lenmed Health Group, is a prominent voice in South Africa’s private healthcare sector. With more than three decades of experience, he brings deep insight into hospital management, healthcare systems and patient-centred care. Known for his strategic leadership and operational expertise, Bishop has played a key role in driving sustainable growth and innovation within Lenmed and the broader healthcare industry.
In this Q&A, Mark shares his perspectives on HASA’s role, sector priorities and the future of healthcare in South Africa.
Q: As HASA Deputy Chairperson, what do you see as the organisation’s core contribution to strengthening South Africa’s health system?
A: The private hospital sector plays a vital role by providing essential facilities and capacity for healthcare professionals to deliver quality care. Over the past four decades, private hospitals have expanded bed capacity while public sector capacity has not kept pace with population growth. This helps meet rising demand and relieves pressure on an already overburdened public system. All industry players, providers and funders, will need to consider the best collaborative approach, and the impact this would have for all and not just concentrate on the impact on their own organisations.
Q: What are HASA’s priorities for long-term sustainability of the healthcare sector?
A: Sustainability depends on affordability across both public and private healthcare. Cost drivers are the same, staffing, infrastructure and medical equipment. Improving the utilisation of limited resources across the system is critical to meeting growing healthcare needs.
Q: How do you view the current medical schemes landscape?
A: Medical schemes operate in a challenging environment characterised by stagnant membership, an ageing population, increasing chronic disease and rising costs driven by advances in medical technology. This is a consequence of a raft of incomplete reforms over the years that together have placed a heavy burden on medical scheme members. Rectifying this could take considerable expense off them.
Q: What reforms could improve affordability while maintaining quality?
A: Increasing medical scheme membership would reduce unit costs. Mandatory medical scheme covers for employed individuals, as recommended by, would expand access to care, reduces pressure on public hospitals and support progress towards universal healthcare. This would need to be done with changes to the reimbursement processes for private care, reducing the impact of fee for service and aligning with quality improvements.
Q: Your career spans 30+ years in private healthcare. What have been the most significant shifts?
Over the years, we have seen patients become more informed about their healthcare needs, medical scheme requirements have evolved and the private healthcare landscape change significantly through consolidation in medical aids.
Q: Where do you see the greatest opportunities for collaboration?
A: The private sector has spare capacity that could be used to treat publicly funded patients. Public-private partnerships, shared infrastructure and co-located facilities offer opportunities to reduce waiting times, lower costs and improve access to care. The caution, is that this needs to align with a national strategy to increase the rate at which nurses are trained, the reality is that both public and private sectors struggle to do the limited professional nurse resources.
Q: What motivates you about your role at Lenmed?
A: Lenmed’s vision of building healthier, more prosperous communities resonates with me. Our hospitals maintain a strong community focus, rooted in the founding of Lenmed Ahmed Kathrada Private Hospital over 40 years ago. Private healthcare is at a tipping point and collaboration across the sector will be essential to grow access and create a sustainable, high-quality healthcare system.