Only about 30% of US adults have spoken with their health care professional about the adverse effects some over-the-counter (OTC) pain relievers can have on blood pressure. The findings are part of a recent online poll commissioned by the American Heart Association.
“It’s paramount that people who have high blood pressure, or are at risk for it, understand the effects associated with some over-the-counter pain relievers,” said Mitchell S. V. Elkind, MD, MS, FAHA, chief clinical science officer of the American Heart Association and a tenured professor of neurology and epidemiology at Columbia University. “A conversation with a health care professional about pain relief options is essential to preventing and managing high blood pressure.”
High blood pressure affects almost half of all people in the US. According to the American Heart Association’s recent poll, of those who have been diagnosed with high blood pressure, white and Asian adults (40%) are significantly less likely than Black (54.2%) and Hispanic (54.1%) adults to have ever discussed the effect some pain relievers have on blood pressure with a health care professional. “Some over-the-counter pain relievers are safer than others,” added Elkind. “A conversation with a health care professional regularly about medications you or a loved one takes is an important step in finding safe options and controlling blood pressure.”
The poll conducted by Big Village, a collaborative and consultative research firm, also looked at how often people used OTC pain relievers. Of the close to 3000 US adults aged 18 and older surveyed, nearly 50% took medication for pain once a week or more. Adults aged 45-54 take them most frequently of all age groups polled. Additional findings include:
Gen X, people born from 1965 to 1980, are significantly more likely than other generations to take OTC pain relievers multiple times a day, but only 41% of Gen X would initially ask a health care professional for alternative pain relief even if they knew some OTC pain relievers can raise a person’s blood pressure.
Gen Z, people born from 1997 to 2012, are significantly less likely (30.5%) than any other generation to initially ask their health care professional for alternative pain relief if they knew some OTC pain relievers can raise a person’s blood pressure.
61% of all respondents had not discussed the effect some over-the-counter pain relievers have on blood pressure with a health care professional.
22% would research an alternative pain reliever online, second only to discussing with a health care professional.
Snoozing, or using intermittent alarms to get in a few more minutes of sleep in the morning, may have benefits for some people, according to research published in the Journal of Sleep Research.
In a study of 1732 adults who described their waking habits, 69% of participants reported using the snooze function or setting multiple alarms at least “sometimes.” In those who snoozed, the average time spent snoozing per morning was 22 minutes, ranging from 1 to 180 minutes. Snoozers tended to be younger than non-snoozers and were more likely to be evening types. Morning drowsiness and shorter sleep were also more common in those who snoozed.
In a second study of 31 habitual snoozers, 30 minutes of snoozing improved or did not affect performance on cognitive tests directly upon rising compared with waking up abruptly. Snoozing resulted in about 6 minutes of lost sleep, but it prevented awakening from slow-wave sleep. There were no clear effects of snoozing on stress hormone levels, morning sleepiness, mood, or overnight sleep structure.
“The findings indicate that there is no reason to stop snoozing in the morning if you enjoy it, at least not for snooze times around 30 minutes. In fact, it may even help those with morning drowsiness to be slightly more awake once they get up,” said corresponding author Tina Sundelin, PhD, of Stockholm University.
When you think of Japan in the age of COVID, you might imagine a crowd of people wearing masks. But many of them are still wearing masks after the pandemic has ended. In an article published this month in the International Journal of Disaster Risk Reduction, a researcher from Osaka University analysed mask use before and after the government of Japan downgraded the legal status of COVID. Results showed that many people continue to wear masks for socio-psychological reasons – including reasons related to ‘relief’ and ‘norm’.
Of course, the obvious motivation for mask use is disease prevention. In the first half of 2020, masks were recommended worldwide because they help to prevent COVID transmission. Japan has since had one of the highest rates of mask usage throughout the pandemic.
However, on May 5, 2023, the World Health Organization declared the end of COVID as a global health emergency. Furthermore, on May 8, Japan downgraded the legal status of COVID to the same level as seasonal influenza.
Michio Murakami, the study’s author, notes, “The online survey shows that 59% of Japanese participants are still wearing masks, even after the downgrading of the legal status of COVID. That is only slightly down from 67%, which was before the downgrading.”
The surveys were conducted among people aged 20 to 69 in Japan. The first survey was performed in April 2023, before the policy changes, while the second was performed after the changes in June 2023. A total of 291 participants completed both surveys.
So what reasons, besides disease prevention, might lead people to continue wearing masks? “One common socio-psychological reason involves what we call ‘relief’. This means that wearing a mask can help relieve anxiety for many people,” explains Murakami. “There’s a second sociological reason, too: a ‘norm’. This refers to when people think they should wear a mask because they see others wearing masks,” he explains. People that have this trait are more likely to wear a mask when others around them are wearing masks, unsurprisingly.
Murakami was also able to document correlations between mask-usage motivations and actual mask usage. For instance, citing psychological reasons for mask use in April was correlated with actually wearing a mask later on in June. Furthermore, wearing a mask in April was associated with citing infection avoidance as a reason to wear masks in June.
“So many Japanese people prefer to wear masks,” notes Murakami. “This study helps us understand why people might do so, even in light of reduced infection risk.”
An international study led by the University of Granada (UGR) has identified for the first time the optimal number of steps at which most people obtain the greatest benefits. The findings, published in the Journal of the American College of Cardiology, also show that walking pace provides additional benefits.
The idea that you should take 10 000 steps a day originated in Japan in the 1960s, but with no scientific basis – rather it is a popular number there. Researchers have now shown that, focusing on cardiovascular disease mortality, most of the benefits are seen at around 7000 steps.
The study provided the first scientific proof for how many steps you need to take per day to significantly reduce the risk of premature death: 8000. Given the average length of a human stride (76cm for men and 67cm for women), taking 8000 steps is equivalent to walking approximately 6.4km a day.
Researchers have also shown that the pace at which we walk has additional benefits, and that it is better to walk fast than slow. With regard to the risk of dying from cardiovascular disease, most of the benefits are seen at around 7000 steps.
The study identifies for the first time the optimal number of steps at which most people obtain the greatest benefits, and also shows that the pace at which you walk provides additional benefits.
The research was carried out in collaboration between researchers from the Netherlands (Radboud University Medical Center), Spain (Universities of Granada and Castilla-La Mancha) and the United States (Iowa State University).
“Traditionally, many people thought that you had to reach about 10 000 steps a day to obtain health benefits – an idea that came out of Japan in the 1960s but had no basis in science,” explains the lead author of the study, Francisco B. Ortega, a professor at the UGR’s Department of Physical Education and Sports.
Previously, no scientific basis
In Japan and China, the number 10 000 is a significant number, being the largest order of magnitude for common usage and also expressing the idea of ‘unending’. The Japanese cheer of banzai literally translates as ‘ten thousand years’.
For instance, the first pedometer marketed to the general public was the “10 000 steps meter” (a literal translation), but the figure had no scientific basis. “We’ve shown for the first time that the more steps you take, the better, and that there is no excessive number of steps that has been proven to be harmful to health,” says Ortega, who also points out that reaching 7000–9000 steps a day is a sensible health goal for most people.
The researchers conducted a systematic literature review and meta-analysis of data from twelve international studies involving more than 110 000 participants.
The results of this study are in line with other recent studies, which show that health benefits are obtained at less than 10 000 steps. “What makes our study different is that, for the first time, we set clear step targets,” explains Esmée Bakker, currently a Marie Curie Postdoctoral Research Fellow at the University of Granada and one of the lead authors of the study.
“In this study, we show that measurable benefits can be obtained with small increases in the number of steps per day, and that for people with low levels of physical activity, every additional 500 steps improves their health. This is good news because not everyone can walk almost 9000 steps a day, at least not at first, so you can set small, reachable goals and gradually make progress and increase the number of steps per day,” the researchers note.
The study revealed no difference between men and women. It also found that faster walking is associated with a reduced risk of mortality, regardless of the total number of steps per day. Additionally, according to Bakker, “it doesn’t matter how you count your steps, whether you wear a smartwatch, a wrist-based activity tracker or a smartphone in your pocket: the step targets are the same.”
Physical activity recommendations: steps
So, should we stop walking when we reach around nine thousand steps? “Absolutely not,” insists Francisco B. Ortega. “More steps are never bad. Our study showed that even as many as 16 000 steps a day does not pose a risk; on the contrary, there are additional benefits compared to walking 7000–9000 steps a day, but the differences in risk reduction are small. Furthermore, the step target should be age appropriate, with younger people being able to set a higher target than older people. It is also important to note that our study only looked at the effect on the risk of all-cause mortality and cardiovascular disease. There are other studies and a large body of scientific evidence that show that doing moderate and even vigorous physical activity is associated with many health benefits, including improvements in sleep quality and mental health, among many others.”
“Our study gives people clear and easily measurable goals,” Bakker continues. “The (inter)national physical activity recommendations advise adults to get 150–300 minutes of moderate-intensity exercise per week. But most people don’t know what exercises count as moderate intensity, making it difficult to verify their compliance with this exercise standard. Counting steps is much simpler, especially since most people have a smartphone or smartwatch these days. Herein lies the importance of our study: to provide simple and concrete targets for the number of daily steps that people can easily measure with their phones and smartwatches or wristbands, and thereby contribute to people’s health,” the authors conclude.
By Matshidiso Lencoasa and Dominic Brown for Spotlight
In the context of weak economic growth, lower-than-expected tax revenues, and the implementation of measures to reduce public spending, there is “rising panic” ahead of this year’s Medium Term Budget Policy Statement (MTBPS). The concern for health care provision is palpable as anticipated budget cuts threaten the country’s already fragile and understaffed public healthcare system. There is only one nurse for every 224 patients in the public health system, and over 5 000 nursing posts remain unfilled (something primarily attributed to funding constraints).
In times of poor economic performance, difficult policy choices and trade-offs arise, and it may be tempting for fiscal policymakers to slash public health spending. However, without meaningful consideration of the impact of these decisions on our people and our constitutional right to access healthcare, the MTBPS risks exacerbating the hardships faced in our country.
Austerity context
South Africa’s economic outlook has been riddled with challenges permeating our healthcare system. Over the past decade, the country’s economic growth has underperformed, falling in real terms from 2.3% in 2013 to 0.1% in 2023. National Treasury has responded to this with cuts to social spending, including healthcare. Public health is receiving fewer resources in real terms, and our government spends more on debt-servicing (R340.5 billion in the 2023/24 Budget) than on healthcare (R259.2 billion in the 2023/24 Budget). Moreover, healthcare’s allocation of R259 billion in 2023/24 was the same as last year’s allocation, meaning that the value of resources allocated to healthcare this year is eroded by Consumer Price Index (CPI) inflation, which was projected to be 4.9% at the time of the Budget Speech in February this year.
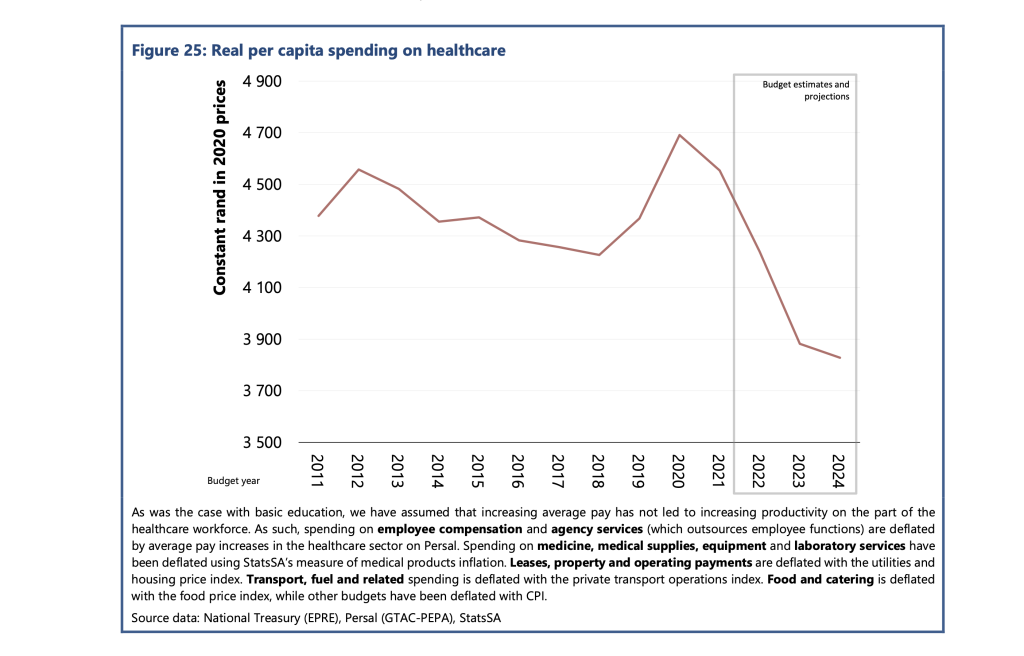
According to the Public Economy Project, the spending per healthcare user fell from approximately R4 600 in 2012 to R4 300 in 2018. PHOTO: Sourced from the Public Economy Project (PEP) Public services, government employment and the budget
Worse, this allocation needed to account for the rising demand projected for public healthcare services. Currently, about 84% of the population relies on the public health care system. This figure is projected to increase in response to population growth and rising unemployment making medical aid inaccessible for many in the country.
According to the Public Economy Project, after accounting for inflation and population growth, the spending per healthcare user fell from approximately R4600 in 2012 to R4300 in 2018. Based on current budget estimates, it is projected that real per capita public health spending will fall below R3 900 by 2024/25.
Implications for health care staffing
Although the 2023/24 budget proposed a measly 1.5% nominal increase to the public sector wage bill, President Cyril Ramaphosa approved a 3.8% increase for this year. However, Treasury’s cost containment measures have stipulated a hiring freeze for the rest of the 2023/24 financial year and no further allocations towards personnel expenditure. This is despite the Department of Health’s 2030 Human Resources for Health Strategy quantifying that 96 586 additional health workers are required to bolster the healthcare of all provinces to the same standard as the third-ranked province by 2025. This requires an additional cost of nearly R40 billion in total.
The real-life implications for South Africans are dire. Chris Hani Baragwanath Hospital – the largest hospital in Africa and the third largest hospital globally – faces significant staff shortages, cancelling almost 900 surgeries in 2022. The underpaid and overworked Chris Hani Baragwanath Hospital nurses have reported “pooling funds to buy patients bread.” Doctors at Nelson Mandela Bay’s Livingstone Tertiary Hospital have attributed “suboptimal, undignified patient care” to budget shortages and forecast higher medico-legal claims, which National Treasury described as a “sub-national risk”. However, budget measures that impede public health care’s ability to address staff shortages exacerbate the likelihood of errors by overstretched staff, worsening the medico-legal claims bill for health departments.
Gender and budget cuts
Health budget cuts disproportionately burden women. This burden is evident in the inordinate risk and prevalence of HIV that women face in the country. It is exacerbated by women’s higher and differentiated health needs (including those for reproductive and maternal health). Women-led households are 40% poorer, and unemployment is most prevalent among women. These socioeconomic factors make women more dependent on the public health system.
Budget cuts and underspending clearly have implications for gender equity in the country.
Furthermore, the Department of Health has recognised the healthcare workforce as a critical driver of inclusive economic growth and a means to create decent work for women, especially in rural and underserved communities. Over 90% of nurses in our public health system are women, and in our society of unequal gendered norms, it is also women who carry the care work burden in the home. Many will likely interpret any proposed MTBPS cuts without factoring gender equity implications as an under-appreciation of women’s labour in making a fragile healthcare system and society work.
A case for human rights budgeting
Although improving the country’s economic outlook is imperative, without consideration of the power that fiscal policy has in advancing human rights in the country, there is a likelihood of tabling an MTBPS that impedes the realisation of constitutionally guaranteed human rights in the country.
More than ever, our health system requires inculcation of human rights impact assessments as recommended by the UN Committee on Economic, Social and Cultural Rights, to which South Africa is a party. These assessments could compel policymakers to outline how the resources allocated will protect the right to access healthcare for all in the country, especially when budget cuts are considered. Including these considerations in budget policy may further advance meaningful public participation processes in fiscal policy.
Furthermore, a gender-responsive MTBPS is long overdue and a powerful means to protect the most vulnerable people in the country from reduced social investment. The health budget could be tagged to identify programmes with gender as a principal or significant objective and areas which would need to be protected and consideration of the gendered experience of healthcare to prevent fiscal policy from worsening gender inequities in the country. Budget policymakers should further promote the collection of gender-disaggregated data and establish indicators and benchmarks on gender and other socio-economic factors to advance a more equitable funding allocation.
Lastly, authentic public engagement will allow National Treasury and budget policymakers to solicit and table more equitable fiscal expansion alternatives. Increased public consultation could include extending the pre-budget consultations with the public.
Moreover, civil society organisations like the Institute of Economic Justice and the Alternative Information and Development Centre (AIDC) have proposed alternative approaches to fiscal constraints that could ensure sufficient resources to protect our frail public health system from threats to resource availability. These alternatives should be explored.
One strategy proposed is strengthening the country’s capacity to halt the significant revenue losses owing to to corporate tax abuses, including illicit financial flows (IFF) and base erosion and profit shifting (BEPS). IFF refers to the cross-border movement of illegally sourced funds while BEPS refers to when multinational companies shift the profits generated in South Africa to another jurisdiction that has lower or zero tax rates in order to minimise their tax burden.
The Financial Intelligence Centre estimates that between $15 billion and $25 billion is shifted out of our country to tax havens yearly. We call for greater urgency towards implementing publicly disclosed beneficial ownership registries based on country-by-country reporting and the automatic exchange of information, strengthening capital and exchange controls, and increasing South African Revenues Services (SARS) capacity to investigate corporations suspected to be involved in IFF and BEPS. These essential measures can contribute to curbing profit shifting, resulting in more than R100 billion in revenue each year.
The upcoming MTBPS will find National Treasury in a challenging position where various trade-offs will likely be made. In this harsh economic climate, if something has to give, it cannot be the constitutional right to health care for all in this country.
*Lencoasa is a Budget Researcher at SECTION27 and Steering Committee Member of the Budget Justice Coalition. Brown is Director of the Alternative Information and Development Centre and member of the Budget Justice Coalition.
Researchers at the Institute of Basic Science (IBS) in South Korea have developed a novel approach to healing muscle injury by employing an ‘injectable tissue prosthesis’ in the form of conductive hydrogels and combining it with a robot-assisted rehabilitation system. They describe their research in a recent publication in the journal Nature.
A large wound such as a shark bite, with the loss of muscle and nerve in the wound cavity, results in a complete loss of motor/sensor function in the leg. If left untreated, such severe muscle damage would result in permanent loss of function and disability.
Traditional rehabilitation methods for these kinds of muscle injuries have long sought an efficient closed-loop gait rehabilitation system that merges lightweight exoskeletons and wearable/implantable devices. Such assistive prosthetic system is required to aid the patients through the process of recovering sensory and motor functions linked to nerve and muscle damage.
Unfortunately, the mechanical properties and rigid nature of existing electronic materials render them incompatible with soft tissues. This leads to friction and potential inflammation, stalling patient rehabilitation.
To overcome these limitations, the IBS researchers turned to a material commonly used as a wrinkle-smoothing filler, called hyaluronic acid. Using this substance, an injectable hydrogel was developed for ’tissue prostheses’, which can temporarily fill the gap of the missing muscle/nerve tissues while it regenerates. The injectable nature of this material gives it a significant advantage over traditional bioelectronic devices, which are unsuitable for narrow, deep, or small areas, and necessitate invasive surgeries.
Thanks to its highly ’tissue-like’ properties, this hydrogel seamlessly interfaces with biological tissues and can be easily administered to hard-to-reach body areas without surgery. The reversible and irreversible crosslinks within the hydrogel adapt to high shear stress during injection, ensuring excellent mechanical stability. This hydrogel also incorporates gold nanoparticles, which gives it decent electrical properties. Its conductive nature allows for the effective transmission of electrophysiological signals between the two ends of injured tissues. In addition, the hydrogel is biodegradable, removing the need for additional surgery.
With mechanical properties akin to natural tissues, exceptional tissue adhesion, and injectable characteristics, researchers believe this material offers a novel approach to rehabilitation.
Next, the researchers put this novel idea to the test in rodent models. To simulate volumetric muscle loss injury, a large chunk of muscle has been removed from the hind legs of these animals. By injecting the hydrogel and implanting the two kinds of stretchable tissue-interfacing devices for electrical sensing and stimulation, the researchers were able to improve the gait in the ‘injured’ rodents. The hydrogel prosthetics were combined with robot assistance, guided by muscle electromyography signals. Together, the two helped enhance the animal’s gait without nerve stimulation. Furthermore, muscle tissue regeneration was effectively improved over the long term after the conductive hydrogel was used to fill muscle damage.
The injectable conductive hydrogel developed in this study excels in electrophysiological signal recording and stimulation performance, offering the potential to expand its applications. It presents a fresh approach to the field of bioelectronic devices and holds promise as a soft tissue prosthesis for rehabilitation support.
Emphasizing the significance of the research, Professor SHIN Mikyung notes, “We’ve created an injectable, mechanically tough, and electrically conductive soft tissue prosthesis ideal for addressing severe muscle damage requiring neuromusculoskeletal rehabilitation. The development of this injectable hydrogel, utilizing a novel cross-linking method, is a notable achievement. We believe it will be applicable not only in muscles and peripheral nerves but also in various organs like the brain and heart.”
Professor SON Donghee added, “In this study, the closed-loop gait rehabilitation system entailing tough injectable hydrogel and stretchable and self-healing sensors could significantly enhance the rehabilitation prospects for patients with neurological and musculoskeletal challenges. It could also play a vital role in precise diagnosis and treatment across various organs in the human body.”
The research team is currently pursuing further studies to develop new materials for nerve and muscle tissue regeneration that can be implanted in a minimally invasive manner. They are also exploring the potential for recovery in various tissue damages through the injection of the conductive hydrogel, eliminating the need for open surgery.