A painful inflammatory form of arthritis, gout is characterised by urate crystals accumulating in joints, soft tissue and bones. To decrease blood urate levels in patients and reduce flareups, the standard treatment is xanthine oxidase inhibitors such as febuxostat. But new research published in Arthritis & Rheumatology has found a possible better option in the form of low doses of benzbromarone, a less commonly used drug.
Biochemically, gout is characterised by extracellular fluid urate saturation, which is reflected by hyperuricaemia in the blood, with plasma or serum urate concentrations in excess of 6.8 mg/dL; this is the approximate limit of urate solubility.
Benzbromarone is a uricosuric drug that has been used in the treatment of gout over the last 30 years. It reduces the urate reabsorption, diminishing serum urate levels and therefore preventing gout flares.
In this prospective single-centre, open-labelled trial, 196 men with gout and low urinary excretion of uric acid were randomised to receiving either low-dose benzbromarone (LDBen) or low-dose febuxostat (LDFeb) for 12 weeks.
More participants in the LDBen group achieved the blood urate target of < 6 mg/dL than those in the LDFeb group (61% versus 32%). There was little difference in side effects between the groups.
The authors concluded that, “The results suggest that low dosing of benzbromarone may warrant stronger consideration as a safe and effective therapy to achieve serum urate target in gout.”
Scientists have now uncovered how the innate immune system detects even very small amounts of HIV-1.The findings, published in Molecular Cell, reveal a two-step molecular strategy that jolts the innate immune response into action when exposed to HIV-1. This has important implications for developing new HIV treatments and vaccines, as well as helping understand the innate immune response in other contexts such as Alzheimer’s.
“This research delineates how the immune system can recognise a very cryptic virus, and then activate the downstream cascade that leads to immunological activation,” says Sumit Chanda, PhD, professor in the Department of Immunology and Microbiology. “From a therapeutic potential perspective, these findings open up new avenues for vaccines and adjuvants that mimic the immune response and offer additional solutions for preventing HIV infection.”
The innate immune system is activated before the adaptive immune system, which is the body’s secondary line of defense that involves more specialised functions, such as generating antibodies. One of the innate immune system’s primary responsibilities is recognizing between “self” (our own proteins and genetic material) and foreign elements (such as viruses or other pathogens). Cyclic GMP-AMP synthase (cGAS) is a key signaling protein in the innate immune system that senses DNA floating in a cell. If cGAS does detect a foreign presence, it activates a molecular pathway to fight off the invader.
However, because HIV-1 is an RNA virus, it produces very little DNA – so little, in fact, that scientists have not understood how cGAS and the innate immune system are able to detect it and distinguish it from our own DNA.
Scripps Research scientists discovered that the innate immune system requires a two-step security check for it to activate against HIV-1. The first step involves a protein called polyglutamine binding protein 1 (PQBP1), which recognises the HIV-1 outer shell as soon as it enters the cell and before it can replicate. PQBP1 then coats and decorates the virus, acting as an alert signal to summon cGAS. Once the viral shell begins to disassemble, cGAS activates additional immune-related pathways against the virus.
The researchers were initially surprised to find that two steps are required for innate immune activation against HIV-1, as most other DNA-encoding viruses only activate cGAS in one step. This is a similar concept to technologies that use two-factor authentication, such as requiring users to enter a password and then respond to a confirmation email.
This two-part mechanism also opens the door to vaccination approaches that can exploit the immune cascade that is initiated before the virus can start to replicate in the host cell, after PQBP1 has decorated the molecule.
“While the adaptive immune system has been a main focus for HIV research and vaccine development, our discoveries clearly show the critical role the innate immune response plays in detecting the virus,” said Sunnie Yoh, PhD, first author of the study and senior staff scientist in Chanda’s lab. “In modulating the narrow window in this two-step process – after PQBP1 has decorated the viral capsid, and before the virus is able to insert itself into the host genome and replicate – there is the potential to develop novel adjuvanted vaccine strategies against HIV-1.”
By shedding light on the workings of the innate immune system, these findings also illuminate how our bodies respond to other autoimmune or neurodegenerative inflammatory diseases. For example, PQBP1 has been shown to interact with tau – the protein that becomes dysregulated in Alzheimer’s disease – and activate the same inflammatory cGAS pathway. The researchers will continue to investigate how the innate immune system is involved in disease onset and progression, as well as how it distinguishes between self and foreign cells.
A study published in Metabolic Brain Disease has established a clear link between mice being fed a high-fat diet for 30 weeks, resulting in diabetes, and a subsequent worsening of their cognitive abilities. This included developing anxiety, depression and worsening Alzheimer’s disease.
Mice with impaired cognitive function were also more likely to gain excessive weight due to poor metabolism caused by brain changes.
Neuroscientist and biochemist Associate Professor Larisa Bobrovskaya, who co-led the study said that the research adds to the growing body of evidence linking chronic obesity and diabetes with Alzheimer’s disease.
“Obesity and diabetes impair the central nervous system, exacerbating psychiatric disorders and cognitive decline. We demonstrated this in our study with mice,” said Associate Prof Bobrovskaya.
In the study, mice were randomised to a standard diet or a high-fat diet for 30 weeks, starting at eight weeks of age. Food intake, body weight and glucose levels were monitored at different intervals, along with glucose and insulin tolerance tests and cognitive dysfunction.
The mice on the high-fat diet gained significant weight, developed insulin resistance and started behaving abnormally compared to those fed a standard diet.
Genetically modified Alzheimer’s disease mice showed a significant deterioration of cognition and pathological changes in the brain while fed the high fat diet.
“Obese individuals have about a 55 per cent increased risk of developing depression, and diabetes will double that risk,” Assoc Prof Bobrovskaya said.
“Our findings underline the importance of addressing the global obesity epidemic. A combination of obesity, age and diabetes is very likely to lead to a decline in cognitive abilities, Alzheimer’s disease and other mental health disorders.”
High dose inhaled nitric oxide gas (iNO) is a safe and effective respiratory therapy for pregnant women hospitalised with severe COVID pneumonia, resulting in faster weaning from oxygen and shorter hospital stay, according to a study published in Obstetrics & Gynecology. Massachusetts General Hospital (MGH) researchers reported that the addition of twice-daily nitric oxide to standard of care oxygen therapy decreased the respiratory rate of pregnant women with low oxygenation levels of the blood without causing any side effects.
“To date, very few respiratory treatments to complement supplemental oxygenation in COVID pregnant patients have been tested,” explained the study’s senior author, Lorenzo Berra, MD. “Investigators from all four medical centers that participated in our study agreed that administration of high dose nitric oxide through a snug-fitting mask has enormous potential as a new therapeutic strategy for pregnant patients with COVID.”
Pneumonia triggered by COVID is particularly threatening to pregnant women since it may quickly progress to hypoxaemia, requiring hospitalisation and cardiopulmonary support. “Compared to non-pregnant female patients with COVID, pregnant women are three times more likely to need intensive care unit admission, mechanical ventilation, or advanced life support, and four times more likely to die,” noted lead author Carlo Valsecchi, MD. “They also face a greater risk of obstetric complications such as preeclampsia, preterm delivery, and stillbirth.”
Nitric oxide is a therapeutic gas that was initially approved by the U.S. Food and Drug Administration in 1999 for inhalation treatment of intubated and mechanically ventilated newborns with hypoxic respiratory failure. With MGH driving many early studies, iNO in high concentrations was also shown to be effective as an antimicrobial in reducing viral replication of SARS-CoV-1 and, more recently, SARS CoV-2. During the first wave of COVID, MGH treated six non-intubated pregnant patients with iNO at high doses of up to 200 parts per million (ppm). Favourable outcomes with iNO led MGH clinicians to offer this treatment to other pregnant patients, and motivated the present study.
Researchers and clinicians from multiple departments in four hospitals – including critical care medicine, respiratory care, and maternal foetal medicine – studied 71 pregnant patients with severe COVID pneumonia admitted to these hospitals, 20 of whom received iNO200 twice daily. The study found that iNO therapy at this dosage, when compared to standard of care alone, resulted in reductions in the need for supplemental oxygen and in hospital and ICU lengths of stay. No adverse events related to the intervention were reported in either mothers or their babies.
“Being able to wean patients from respiratory support quicker could have other profound implications, including reducing stress on women and their families, lowering the risk of hospital-acquired infections, and relieving the burden on the health care system,” noted Dr Berra. “Above all, our study supports the safety of high dose nitric oxide in the pregnant population, and we hope more physicians will consider incorporating it into carefully monitored treatment regimens.”
In the past year, the Commission for Conciliation, Mediation and Arbitration (CCMA) has delivered several arbitration awards which have upheld the dismissals of employees who refused to get vaccinated against COVID.
But a recent award has created some confusion about whether this is still allowed and under what circumstances.
On 22 June, CCMA Commissioner Richard Byrne found that it was unfair and unconstitutional for Baroque Medical, which supplies and sells medical equipment, to retrench Kgomotso Tshatshu for refusing to get a Covid vaccination. The company was ordered to pay her 12 months’ salary as compensation (the maximum allowed).
But this contradicts an earlier CCMA award by Commissioner Piet van Staden, delivered in May, who found that Baroque Medical was within its rights to retrench another employee, Cecilia Bessick, who had also refused to get a COVID vaccine.
These conflicting decisions may be understandable, because CCMA arbitration awards do not create binding legal precedent in the same way as court judgments. The most recent CCMA ruling therefore does not set a binding legal precedent that employees cannot be dismissed for refusing to get a COVID vaccine.
The Labour Court has also not yet delivered any binding judgment about whether an employer can fairly dismiss an employee who refuses to get a Covid vaccination. Until this occurs, it is likely the CCMA will continue to give conflicting decisions about whether employers can fairly dismiss employees who refuse to get a vaccine.
Below, we explain what the law currently says about whether an employee can be dismissed for refusing to get a COVID vaccine and under what circumstances.
Labour Relations Act
The Labour Relations Act (LRA) says that an employee can only be dismissed for these reasons: when they are guilty of misconduct; suffer from an incapacity, such as ill health or injury, which prevents them from performing their duties; have to be retrenched because of the economic, structural, technological or similar needs of their employer.
The LRA also requires an employer to follow a fair procedure before dismissing an employee. Usually, this would involve explaining to an employee why they could be dismissed if they refuse to get a Covid vaccine and give the employee an opportunity to explain why they should not be dismissed.
The LRA, however, does not explain whether an employee who refuses to get vaccinated can be dismissed for misconduct or incapacity. The LRA also does not explain whether an employee who refuses to get a Covid vaccine can be retrenched.
Occupational Health and Safety Act
But the Occupational Health and Safety Act does require employers to take all reasonable steps to provide their employees with a safe and healthy working environment. The act also requires employers to take reasonable steps to ensure other people who may be affected by their business activities (such as customers or suppliers) are not exposed to a hazard to their health or safety – such as Covid.
During March, the Minister of Labour issued a Code of Good Practice which explains the steps that an employer should take to manage Covid in their workplace and to comply with their legal duties to provide a safe and healthy working environment.
This code was enacted after a previous directive on managing Covid in the workplace was repealed after the State of Disaster came to an end.
Code of Good Practice
According to the new Code of Good Practice, every employer with at least 20 employees must conduct a “risk assessment” and must develop a COVID plan with the measures it will implement regarding vaccination of employees and when they should be fully vaccinated. When developing the plan, the employer must consult with any representative trade union in its workplace or an employee representative.
The risk assessment and plan, among other things, should identify employees who must be vaccinated and must notify them of their duty to get a vaccination.
The code also states employers can require employees to disclose their vaccination status and to produce a vaccine certificate in order to give effect to the code.
The code further states that employees can lawfully refuse work when there exists a serious risk that they may imminently be exposed to COVID in the workplace. Should this occur, the employer cannot take any action against that employee for refusing to work, such as later dismissing or suspending them from work.
There may be situations where a refusal by employees to work because other employees refuse to get vaccinated, could justify the dismissal of the employees who refuse to get a COVID vaccine. This is because the refusal of many employees to work could affect the ability of a company or business to operate. This could potentially justify retrenchment of employees who refuse to get a COVID vaccine.
However, should an employee refuse to get vaccinated, the code also says that the employer should take steps to reasonably accommodate them in a position that does not require them to be vaccinated. Should an employee produce a valid medical certificate, which provides legitimate reasons why they cannot be vaccinated, the employer can send that employee to another doctor at their own expense.
The code does recognise that it would be unfair to dismiss employees who cannot be vaccinated on valid medical grounds. But, the duty to accommodate employees who refuse to get vaccinated on other grounds would depend on whether an employer has another position available which does not require that employee to be vaccinated. Should the employer not have an alternative position which does not require the employee to be vaccinated, this could be a fair reason to dismiss them.
It is important to note that the code does state that it reflects the policy position of the Department of Labour and that it should be applied until any of its provisions are reversed by a court judgment. Until the Labour Court delivers a binding judgment on when employees can be dismissed for refusing to get a COVID vaccination, it would seem it would be best to follow the provisions of the code.
A cross sectional study published in Annals of Internal Medicine uncovered substantial discrepancies between individual estimated glomerular filtration rate (eGFR) and directly measured GFR (mGFR).The authors suggest that eGFR calculations on lab reports also state this distribution of uncertainty, and also that renaming the eGFR as a population average GFR (or paGFR) merits further discussion.
GFR is the standard metric used to assess and monitor kidney function. Directly measured GFR, or mGFR, requires injecting a filtration marker and measuring plasma or urinary clearance by serial blood and urine sampling under standardized conditions is not possible for every patient. So eGFR calculated from serum creatinine is often used by clinicians to predict an mGFR. Population-level discrepancies between eGFR and mGFR are low, but individual discrepancies are much higher. It is important to understand the magnitude of these individual-level differences for clinical decision making.
Researchers calculated eGFR from serum creatinine alone and cystatin C and creatinine using the Chronic Kidney Disease Epidemiology Collaboration equations for 3223 participants and compared their eGFR to their mGFR to quantify the magnitude and consequences of the individual-level differences between the two. The authors found substantial discrepancies between directly measured GFR and estimated GFR, resulting in only about 50% agreement between CKD stages. Individual-level differences between the mGFR and the eGFR did not improve substantially using cystatin C.
The authors suggested that several factors contribute to these discrepancies: creatinine and cystatin C have non-GFR factors influencing their serum concentration; variability in the mGFR can result from normal physiology and measurement error from mGFR markers and technique; and as GFR estimation models the ratio of mGFR–body surface area as a function of serum markers, it incorporates errors in mGFR and errors in body surface area calculated from height and weight.
The authors say that their findings highlight the need to make direct GFR measurements available to patients who need them. They note that implementation studies are needed in this area, and research is needed to assess how the availability and use of mGFRs change clinical management.
A new study published in the journal PLOS ONE has discovered that feeling hungry really can make us ‘hangry’, with emotions such as anger and irritability strongly linked with hunger.
Hangry, a portmanteau of hungry and angry, is a commonly used colloquialism, but the phenomenon has not been widely explored by science outside of laboratory environments.
The study’s researchers found that hunger is associated with increased levels of anger and irritability, as well as reduced levels of pleasure.
The researchers recruited 64 adult participants, who recorded their levels of hunger and various measures of emotional wellbeing over a 21-day period using a smartphone app. They made their reports with the app five times a day, allowing data collection to take place in real-world settings such as at work or at home.
Hunger was found to be linked with stronger feelings of anger and irritability, as well as lower ratings of pleasure, and the effects were substantial, even after taking into account demographic factors such as age and sex, body mass index, dietary behaviour, and individual personality traits.
Hunger was associated with 37% of the variance in irritability, 34% of the variance in anger and 38% of the variance in pleasure recorded by the participants. The research also found that the negative emotions – irritability, anger, and unpleasantness – are caused by both day-to-day fluctuations in hunger, as well as residual levels of hunger measured by averages over the three-week period.
Lead author of the study Viren Swami, Professor of Social Psychology at Anglia Ruskin University (ARU), said: “Many of us are aware that being hungry can influence our emotions, but surprisingly little scientific research has focused on being ‘hangry’.
“Ours is the first study to examine being ‘hangry’ outside of a lab. By following people in their day-to-day lives, we found that hunger was related to levels of anger, irritability, and pleasure.
“Although our study doesn’t present ways to mitigate negative hunger-induced emotions, research suggests that being able to label an emotion can help people to regulate it, such as by recognising that we feel angry simply because we are hungry. Therefore, greater awareness of being ‘hangry’ could reduce the likelihood that hunger results in negative emotions and behaviours in individuals.”
The field work was carried out by Stefan Stieger, Professor of Psychology at Karl Landsteiner University of Health Sciences. Prof Stieger said: “This ‘hangry’ effect hasn’t been analysed in detail, so we chose a field-based approach where participants were invited to respond to prompts to complete brief surveys on an app. They were sent these prompts five times a day at semi-random occasions over a three-week period.
“This allowed us to generate intensive longitudinal data in a manner not possible with traditional laboratory-based research. Although this approach requires a great deal of effort – not only for participants but also for researchers in designing such studies – the results provide a high degree of generalisability compared to laboratory studies, giving us a much more complete picture of how people experience the emotional outcomes of hunger in their everyday lives.”
COVID vaccine acceptance across much of the world increased by 3.7% between 2020 and 2021, according to a new study published in Nature Communications.
In a June 2021 survey of over 23 000 individuals across 23 countries, the researchers found that 75.2% of respondents reported vaccine acceptance, up from 71.5% one year earlier.
The study was carried out during a year of substantial but very unequal global COVID vaccine availability and acceptance, which required new assessments of the drivers of vaccine hesitancy and the characteristics of people not vaccinated.
Vaccine hesitancy was most consistently associated with concerns about vaccine safety and efficacy and mistrust in vaccine development. Other factors associated with vaccine hesitancy varied by country and included personal experience with COVID (eg, sickness or loss of a family member) and demographic characteristics (eg, gender, education, and income).
The authors also found that vaccine hesitancy was not associated with a country’s current COVID case burden and mortality. In June 2021, vaccine hesitancy was reported most frequently in Russia (48.4%), Nigeria (43%), and Poland (40.7%), and least often in China (2.4%), the UK (18.8%), and Canada (20.8%).
“In order to improve global vaccination rates, some countries may at present require people to present proof of vaccination to attend work, school, or indoor activities and events,” said CUNY SPH Senior Scholar Jeffrey Lazarus. “Our results found strong support among participants for requirements targeting international travellers, while support was weakest among participants for requirements for schoolchildren.”
Those who were vaccine-hesitant were also less likely to express support for vaccine mandates. “Importantly, however, recommendations by a doctor, or to a lesser extent by an employer, might have an impact on a respondent’s views on vaccination in some countries,” said CUNY SPH Dean Ayman El-Mohandes.
Although some countries are currently disengaging from evidence-based COVID control measures, the disease has by no means been controlled or ended as a public health threat. The authors note that for ongoing COVID vaccination campaigns to succeed in improving coverage going forward, substantial challenges remain. These include targeting those reporting lower vaccine confidence with evidence-based information campaigns and greatly expanding vaccine access in low- and middle-income countries.
The Role of Social Networks
The researchers also held a meeting to explore vaccine messaging. According to data presented from a European survey carried out by the Vaccine Confidence Project, the population group most exposed to social networks, ie people under 24, with secondary or university studies and living in urban areas, are the most reluctant to be vaccinated. Additionally, messages that call for vaccination as a “moral obligation” are strongly rejected compared to those that call for “protection,” which are more commonly well received.
As with previous studies, humour was shown to be one of the most effective ways to convey anti-vaccine messages. Therefore, participants in the meeting agreed on the need to disseminate the benefits of vaccines using this same tool, but without making fun of those who have mistaken beliefs about vaccines. In the face of misinformation, it is important to improve information on vaccination using simple language and channels that reach the population, such as social networks, the participants concluded.
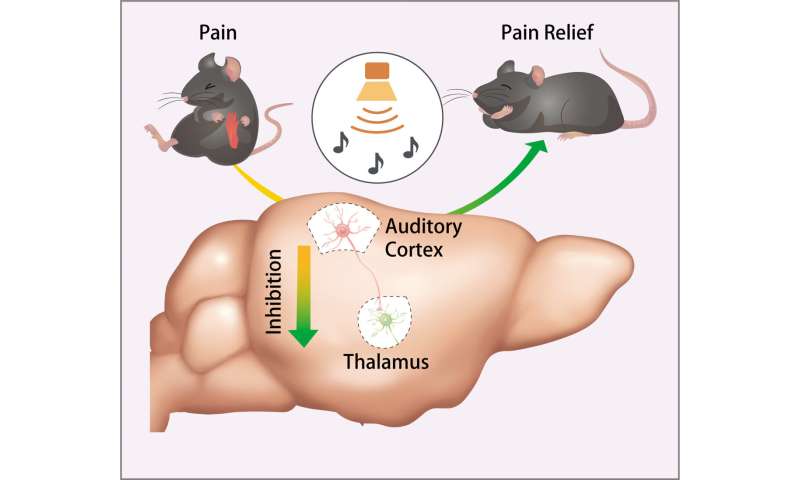
Sound is known to suppress the sensation of pain, and now scientists have identified the neural mechanisms through which sound blunts pain in mice. The findings, which could inform development of safer methods to treat pain in humans, were published in Science.
“We need more effective methods of managing acute and chronic pain, and that starts with gaining a better understanding of the basic neural processes that regulate pain,” said the director of the National Institute of Dental and Craniofacial Research (NIDCR), Rena D’Souza, DDS, PhD. “By uncovering the circuitry that mediates the pain-reducing effects of sound in mice, this study adds critical knowledge that could ultimately inform new approaches for pain therapy.”
Studies as far back as 1960, have shown that music and other kinds of sound can help alleviate acute and chronic pain in humans, including pain from dental and medical surgery, labour and delivery, and cancer. Yet the mechanism behind this remained elusive.
“Human brain imaging studies have implicated certain areas of the brain in music-induced analgesia, but these are only associations,” said co-senior author Yuanyuan (Kevin) Liu, PhD, at NIDCR. “In animals, we can more fully explore and manipulate the circuitry to identify the neural substrates involved.”
The researchers first exposed mice with inflamed paws to three types of sound: a pleasant piece of classical music, an unpleasant rearrangement of the same piece, and white noise. Surprisingly, all three types of sound, when played at a low intensity relative to background noise (about the level of a whisper) reduced pain sensitivity in the mice. Higher volume had no effect on their pain sensitivity.
Inhibition of auditory cortex inputs to the thalamus drives sound-induced analgesia. Credit: Conghuan Ye
“We were really surprised that the intensity of sound, and not the category or perceived pleasantness of sound would matter,” Dr Liu said.
To explore the brain circuitry underlying this effect, the researchers trace connections between brain regions using fluorescent protein-tagged viruses. They identified a route from the auditory cortex to the thalamus, which relays sensory signals, including pain, from the body. In freely moving mice, low-intensity white noise reduced the activity of neurons at the receiving end of the pathway in the thalamus.
Without sound, suppressing the pathway with light- and small molecule-based techniques mimicked the pain-blunting effects of low-intensity noise, while turning on the pathway restored animals’ sensitivity to pain.
Dr Liu said it is unclear if similar brain processes are involved in humans, or whether other aspects of sound, such as its perceived harmony or pleasantness, are important for human pain relief.
“We don’t know if human music means anything to rodents, but it has many different meanings to humans – you have a lot of emotional components,” he said.
The results could give scientists a starting point for studies to determine whether the animal findings apply to humans, and ultimately could inform development of safer alternatives to opioids for treating pain.
Industry-sponsored studies on a new drug or health technology are more likely to be found ‘cost-effective’ than independent studies, across a range of diseases, according to findings from a study published in The BMJ.
In a linked editorial, experts make a call for better reporting of results, more transparency, open-source cost-effectiveness models, and more independent studies, to reduce decision makers’ reliance on potentially biased cost-effectiveness analyses.
A cost-effectiveness analysis (CEA) provided the manufacturer is required by some countries to weigh up a product’s costs and effects.
This cost analysis evidence can be used to set the price for a drug or health technology or decide whether insurance policies will cover them. New drugs covered by insurance plans can be much more profitable than those not covered, which could lead to bias in CEAs funded by the drug and technology manufacturing industry.
While previous studies have consistently shown sponsorship bias in CEAs, most studies were limited to specific diseases, and are out of date. To fill in the gaps, Feng Xie and Ting Zhou from McMaster University, Canada, analysed data from all eligible CEAs published between 1976 and March 2021.
They selected CEAs that reported an incremental cost-effectiveness ratio (ICER) using quality-adjusted life years or QALYs – a ‘value for money’ metric of years lived in good health.
The authors used data from the Tufts Cost-Effectiveness Analysis Registry. In total, 8192 CEAs were included in the study, of which nearly 30% were sponsored by industry.
The study defined CEA industry sponsorship as an analysis funded by drug, medical device, or biotechnology companies, either wholly or in part.
The results show that the industry-sponsored CEAs were significantly more likely to conclude that the new medicine or health technology was cost-effective than those not sponsored by industry.
For example, industry-sponsored studies were more likely to report the intervention being studied as cost-effective below the commonly used threshold of $50 000 per QALY gained than non-industry sponsored studies.
Among 5877 CEAs that reported the intervention was more effective but more expensive than the comparator, the ICERs from industry sponsored studies were one third (33%) lower than those from non-industry sponsored studies.
While only having the registry information to work with was a limitation, the authors said their analysis provides a basis for comparison with previous investigations.
As such, they suggested that “sponsorship bias in CEAs is significant, systemic, and present across a range of diseases and study designs.”
In lower and middle-income countries, industry bias can increase drug prices, where fewer resources mean decision-makers often need to rely on published, rather than independent CEAs.
In a linked editorial, Adam Raymakers at Cancer Control Research, Canada, and Aaron Kesselheim at Brigham and Women’s Hospital, USA, argue that decision-makers “should exercise caution when using published cost-effectiveness analysis in coverage decisions.”
They say finding solutions to tackle bias is more important than ever, and make the case for open-source analysis models, increased transparency, and increased funding for independent analyses, to help minimise reliance on industry-sponsored cost analyses.