In a large-scale study of cancer among 75 000 patients with a diagnosis of diverticular disease and colorectal histopathology, researchers have reported an elevated cancer risk in patients with diverticular disease. Their findings were published in the Journal of the National Cancer Institute.
The data comes from the ESPRESSO cohort, which covers all histopathology reports from Sweden’s 28 pathology departments. Through linkage with the Swedish national patient register, researchers identified patients with diverticular disease. Diverticular disease can present through gastrointestinal bleeding, but also through diverticulitis when patients may have fever, nausea and abdominal pain. Previous research has focused on colorectal cancer development in diverticular disease but less has been know about cancer development elsewhere. The researchers found a 33% increased risk of overall cancer in Swedish patients with diverticular disease.
“This is the first nationwide cohort study to demonstrate that diverticular disease is associated with an increased, long-term risk of overall cancer”, says first-author Wenjie Ma from Massachusetts General Hospital. “Diverticular disease is associated with an increased risk of specific cancers, including liver cancer and lung cancer.”
She also adds that “Given the high prevalence of diverticular disease, our results highlight the need for awareness for cancer, not only for colorectal cancer, in patients with diverticular disease.”
Patients with diverticular disease had significantly increased overall cancer incidence (24.5 vs 18.1 cancer cases per 1000 person-years). After adjusting for covariates, these rates corresponded to 1 extra cancer case in 16 individuals with diverticular disease followed for ten years.
“There has been a lot of research on extraintestinal cancer in other bowel disorders such as inflammatory bowel disease (IBD) and celiac disease, but less is known about diverticular disease”, says senior author Jonas F Ludvigsson, professor at Karolinska Institutet.
“These data suggest that patients with diverticular disease are at increased risk of other cancers than colorectal cancer, but it should also be emphasized that the absolute risk for cancer was moderate”, adds Ludvigsson. “I hope other researchers are inspired by our findings and explore the biological mechanisms underlying the association between diverticular disease and cancer”, he concludes.
A large-scale comparison of direct oral anticoagulants (DOACs), published in Annals of Internal Medicine, one of the two most common direct oral anticoagulants (DOACs), apixaban, has the lowest risk of gastrointestinal bleeding, with similar performance on stroke prevention and other side effects.
DOACs are used to prevent strokes for people with atrial fibrillation, a condition affecting over 33 million people worldwide. They have recently become gained popularity over warfarin, the previous standard treatment, as they do not require as much follow-up monitoring (which was particularly valuable during the COVID pandemic) and have less risk of side-effects.
For the new study, University College London researchers compared the efficacy and risk of side effects for the four most common DOACs. They reviewed data from more than 500 000 new DOAC users in the UK, France, Germany and the US, including 281 320 apixaban users, 61 008 dabigatran users, 12 722 edoxaban users, and 172 176 rivaroxaban users.
They found that all four drugs were comparable on outcomes for ischemic stroke, brain bleeds and all-cause mortality, while they did identify a difference in risk of gastrointestinal bleeding, which is one of the most common and concerning side effects of DOACs.
The study revealed that apixaban stood out as having lower risk of gastrointestinal bleeding, with 19-28% lower risks when compared directly to each of the other three DOACs.
The researchers found that their findings held true when looking at data only from those aged over 80, and those with chronic kidney disease, two groups that are often underrepresented in clinical trials.
Dr Wallis Lau (UCL School of Pharmacy), who jointly led the work along with her colleague Professor Ian Wong, said: “Direct oral anticoagulants have been prescribed with increasing frequency worldwide in recent years, but evidence comparing them directly has been limited. Our results indicate that apixaban may be preferable to other blood thinners because of the lower rate of gastrointestinal bleeding and similar rates of stroke, a finding that we hope will be supported by randomised controlled trials.
“As with all medications, potential risks and benefits can differ between people, so considering the full spectrum of outcomes and side effects will still be necessary for each individual patient.
In mice, researchers have shown that Chlamydia pneumoniae can travel through the olfactory nerve in the nose and into the brain, where it creates markers that are a tell-tale sign of Alzheimer’s disease. Damage from nose picking can make infection easier for C. pneumoniae.
The Griffith University study, published in the journal Scientific Reports, showed that C. pneumoniae used the nerve extending between the nasal cavity and the brain as an invasion path to invade the central nervous system. The cells in the brain then responded by depositing amyloid beta protein which is a hallmark of Alzheimer’s disease.
Professor James St John, Head of the Clem Jones Centre for Neurobiology and Stem Cell Research, is a co-author of the world first research.
“We’re the first to show that Chlamydia pneumoniae can go directly up the nose and into the brain where it can set off pathologies that look like Alzheimer’s disease,” Professor St John said. “We saw this happen in a mouse model, and the evidence is potentially scary for humans as well.”
The olfactory nerve in the nose is directly exposed to air and offers a short pathway to the brain, one which bypasses the blood-brain barrier. It’s a route that viruses and bacteria have sniffed out as an easy one into the brain.
The team at the Centre is already planning the next phase of research and aim to prove the same pathway exists in humans.
“We need to do this study in humans and confirm whether the same pathway operates in the same way. It’s research that has been proposed by many people, but not yet completed. What we do know is that these same bacteria are present in humans, but we haven’t worked out how they get there.”
There are some simple steps to look after the lining of your nose that Professor St John suggests people can take now if they want to lower their risk of potentially developing late-onset Alzheimer’s disease.
“Picking your nose and plucking the hairs from your nose are not a good idea”,” he said.
“We don’t want to damage the inside of our nose and picking and plucking can do that. If you damage the lining of the nose, you can increase how many bacteria can go up into your brain.”
Smell tests may also have potential as detectors for Alzheimer’s and dementia says Professor St John, as loss of sense of smell is an early indicator of Alzheimer’s disease. He suggests smell tests from when a person turns 60 years old could be beneficial as an early detector.
“Once you get over 65 years old, your risk factor goes right up, but we’re looking at other causes as well, because it’s not just age—it is environmental exposure as well. And we think that bacteria and viruses are critical.”
Scientists investigating why people who have had shingles have an increased stroke risk now believe the answer lies within, exosomes, lipid vesicles called that shuttle proteins and genetic information between cells. Their study, published The Journal of Infectious Diseases, details the mechanisms behind the link between shingles and strokes.
“Most people know about the painful rash associated with shingles, but they may not know that the risk of stroke is elevated for a year after infection,” said the study’s lead author Andrew Bubak, PhD, assistant research professor in the Department of Neurology at the University of Colorado School of Medicine. “Importantly, the rash is often completely healed and individuals feel normal but nonetheless are walking around with this significant elevation in stroke risk.”
Herpes zoster (HZ) or shingles is caused by the varicella zoster virus which causes chicken pox. The virus lingers in the ganglionic neurons and can reactivate, causing excruciating pain. But researchers have found that shingles can also increase the risk of stroke especially for those under age 40 where the shingles vaccine is not typically recommended.
The risk is greatest in people with the rashes on their faces, perhaps due to the proximity to the brain.
To better understand how this works, Bubak and his team began looking more closely at exosomes.
“Exosomes carry pathogenic cargo that can cause thrombosis and inflammation distant from site of actual infection,” Bubak said. “That could ultimately lead to a stroke in patients.”
Researchers collected plasma samples from 13 patients with shingles and 10 without. The samples were taken at time of infection and at 3-month follow-ups for a subset of patients and exosomes were extracted from the plasma.
The researchers found prothrombotic exosomes which could cause blood clots in those with the infection. They also discovered proinflammatory exosomes that also pose risks for stroke at the 3-month follow-up.
Bubak said the findings suggest that in a subset of people with shingles, the virus may not return to latency or the circulating exosomes that induce a prolonged prothrombotic state may persist even after therapy is done and the rash is gone. He said using antiviral agents longer with the addition of antiplatelet and anti-inflammatory agents could help.
“As well as initiatives to increase HZ vaccine uptake to decrease stroke risk, particularly in individuals with known preexisting stroke risk factors,” said Bubak. “If these findings are confirmed with a larger longitudinal study, then this could change clinical practice.”
Most physicians are unaware of the connection between shingles (which has an effective vaccine) and stroke.
“But it’s really important and so easily mitigated,” Bubak said. “Send them home with antiplatelet agents.”
Red mitochondria in airway cells become coated with green SARS-COV-2 proteins after viral infection: Researchers discovered that the virus that causes COVID-19 damages lungs by attacking mitochondria. Credit: Stephen Archer
Viruses and bacteria have a very long history. Because viruses can’t reproduce without a host, they’ve been attacking bacteria for millions of years. Some of those bacteria eventually became mitochondria, synergistically adapting to life within eukaryotic cells (cells that have a nucleus containing chromosomes).
Ultimately, mitochondria became the powerhouses within all human cells.
This is the story of how a team, assembled during the pandemic, recognized the mechanism by which these viruses were causing lung injury and lowering oxygen levels in patients: It is a throwback to the primitive war between viruses and bacteria – more specifically, between this novel virus and the evolutionary offspring of bacteria, our mitochondria.
SARS-CoV-2 is the third novel coronavirus to cause human outbreaks in the 21st century, following SARS-CoV in 2003 and MERS-CoV in 2012. We need to better understand how coronaviruses cause lung injury to prepare for the next pandemic.
How COVID-19 affects lungs
People with severe COVID-19 pneumonia often arrive at the hospital with unusually low oxygen levels. They have two unusual features distinct from patients with other types of pneumonia:
First, they suffer widespread injury to their lower airway (the alveoli, which is where oxygen is taken up).
Second, they shunt blood to unventilated areas of the lung, which is called ventilation-perfusion mismatch. This means blood is going to parts of the lung where it won’t get sufficiently oxygenated.
We already knew that mitochondria are not just the powerhouse of the cell, but also its main consumers and sensors of oxygen. Mitochondria control the process of programmed cell death (called apoptosis), and they regulate the distribution of blood flow in the lung by a mechanism called hypoxic pulmonary vasoconstriction.
This mechanism has an important function. It directs blood away from areas of pneumonia to better ventilated lobes of the lung, which optimizes oxygen-uptake. By damaging the mitochondria in the smooth muscle cells of the pulmonary artery, the virus allows blood flow to continue into areas of pneumonia, which also lowers oxygen levels.
It appeared plausible that SARS-CoV-2 was damaging mitochondria. The results of this damage – an increase in apoptosis in airway epithelial cells, and loss of hypoxic pulmonary vasoconstriction – were making lung injury and hypoxaemia (low blood oxygen) worse.
Our discovery, published in Redox Biology, explains how SARS-CoV-2, the coronavirus that causes COVID-19 pneumonia, reduces blood oxygen levels.
We show that SARS-CoV-2 kills airway epithelial cells by damaging their mitochondria. This results in fluid accumulation in the lower airways, interfering with oxygen uptake. We also show that SARS-CoV-2 damages mitochondria in the pulmonary artery smooth muscle cells, which inhibits hypoxic pulmonary vasoconstriction and lowers oxygen levels.
Attacking mitochondria
Coronaviruses damage mitochondria in two ways: by regulating mitochondria-related gene expression, and by direct protein-protein interactions. When SARS-CoV-2 infects a cell, it hijacks the host’s protein synthesis machinery to make new virus copies. However, these viral proteins also target host proteins, causing them to malfunction. We soon learned that many of the host cellular proteins targeted by SARS-CoV-2 were in the mitochondria.
How SARS-CoV-2 targets mitochondria to kill lung cells and prevent oxygen sensing. Credit: Brooke Ring, provided by Stephen Archer
Viral proteins fragment the mitochondria, depriving cells of energy and interfering with their oxygen-sensing capability. The viral attack on mitochondria starts within hours of infection, turning on genes that break the mitochondria into pieces (called mitochondrial fission) and make their membranes leaky (an early step in apoptosis called mitochondrial depolarization).
In our experiments, we didn’t need to use a replicating virus to damage the mitochondria – simply introducing single SARS-CoV-2 proteins was enough to cause these adverse effects. This mitochondrial damage also occurred with other coronaviruses that we studied.
We are now developing drugs that may one day counteract COVID-19 by blocking mitochondrial fission and apoptosis, or by preserving hypoxic pulmonary vasoconstriction. Our drug discovery efforts have already enabled us to identify a promising mitochondrial fission inhibitor, called Drpitor1a.
Our team’s infectious diseases expert, Gerald Evans, notes that this discovery also has the potential to help us understand Long COVID. “The predominant features of that condition – fatigue and neurologic dysfunction – could be due to the lingering effects of mitochondrial damage caused by SARS-CoV-2 infection,” he explains.
Bacteria are regularly attacked by viruses, called bacteriophages, that need a host to replicate in. The bacteria in turn fight back, using an ancient form of immune system called the CRISPR-cas system, that chops up the viruses’ genetic material. Humans have recently exploited this CRISPR-cas system for a Nobel Prize-winning gene editing discovery.
The ongoing competition between bacteria and viruses is a very old one; and recall that our mitochondria were once bacteria. So perhaps it’s not surprising at all that SARS-CoV-2 attacks our mitochondria as part of the COVID-19 syndrome.
Pandemic pivot
The original team members on this project are heart and lung researchers with expertise in mitochondrial biology. In early 2020 we pivoted to apply that in another field – virology – in an effort to make a small contribution to the COVID-19 puzzle.
Our discovery owes a lot to our virology collaborators. Early in the pandemic, University of Toronto virologist Gary Levy offered us a mouse coronavirus (MHV-1) to work with, which we used to make a model of COVID-19 pneumonia. Che Colpitts, a virologist at Queen’s University, helped us study the mitochondrial injury caused by another human beta coronavirus, HCoV-OC43.
Finally, Arinjay Banerjee and his expert SARS-CoV-2 virology team at Vaccine and Infectious Disease Organization (VIDO) in Saskatoon performed key studies of human SARS-CoV-2 in airway epithelial cells. VIDO is one of the few Canadian centres equipped to handle the highly infectious SARS-CoV-2 virus.
Our team’s super-resolution microscopy expert, Jeff Mewburn, notes the specific challenges the team had to contend with.
“Having to follow numerous and extensive COVID-19 protocols, they were still able to exhibit incredible flexibility to retool and refocus our laboratory specifically on the study of coronavirus infection and its effects on cellular/mitochondrial functions, so very relevant to our global situation,” he said.
Our discovery will hopefully be translated into new medicines to counter future pandemics.
Rheumatoid arthritis (RA) is a chronic autoimmune disease that is associated with aberrant immune responses. In a recent analysis published in Arthritis & Rheumatology, people with RA and those at risk for the disease had higher blood levels of antibodies against a protein expressed by Prevotella copri, a common gut bacteria.
The study compared 98 participants with established RA who were compared with 98 controls without the condition, as well as 67 participants at high risk for RA who were compared with 67 controls. The researchers measured levels of antibodies against Pc-p27, a protein expressed by P. copri.
Participants with RA had significantly higher levels of IgA anti-Pc-p27 antibodies and trends towards higher levels of IgG anti-Pc-p27 antibodies when compared to their matched controls. When stratified by early versus established RA, early RA participants had median values of IgG anti-Pc-p27 antibodies that were overall higher, whereas median values of IgA anti-Pc-p27 were statistically significantly higher in participants with established RA, compared with their matched controls.
The authors noted that additional research into the roles of this and other microorganisms in rheumatoid arthritis is warranted.
“Our hope is that these findings can help to further elucidate the complex etiologic role of bacterial commensals in people who are at-risk of developing RA and in those with RA so that targeted therapies can be developed with the goals of providing better treatment and ultimately, prevention of the disease,” said corresponding author Jennifer A. Seifert, MPH, of the University of Colorado Denver.
When dealing with risks, the often-used metric of “deaths per 100 000 population” can be a bit unwieldy, especially when explaining risk to patients. During the COVID pandemic, this became something of a problem when trying to convey the risks of vaccination to the general public. Many felt that the risk of adverse effects outweighed the protection that the vaccination conferred against the coronavirus.
But there is a different, more approachable metric – in 1979, Ronald A. Howard introduced the ‘micromort’ – defined as one chance of death in a million. One in a million is about the same odds as flipping a coin 20 times a row and getting the same result.
Though its name is sure to make some people giggle, the micromort is commonly used in actuarial sciences and decision analyses to quantify the risk of death per unit of exposure to a risk factor or event (Howard, 1980). micromorts have the advantage of being easier to interpret and comprehend than abstract numerical figures, and have been used to convey risks associated with surgical operations and medical treatments.
For example, the mortality risk of general anaesthesia is 10 micromorts per procedure (ie, a 0.001% chance of dying), which is comparable to the mortality risk of an experienced skydiver takes when doing a parachute jump. Chronic cigarette smoking reduces adult life expectancy by 6.5 years on average; said differently, averaged over a lifetime, smoking reduces life expectancy by 7 micromorts per day (3.5 hours per day) (Shaw et al., 2000).
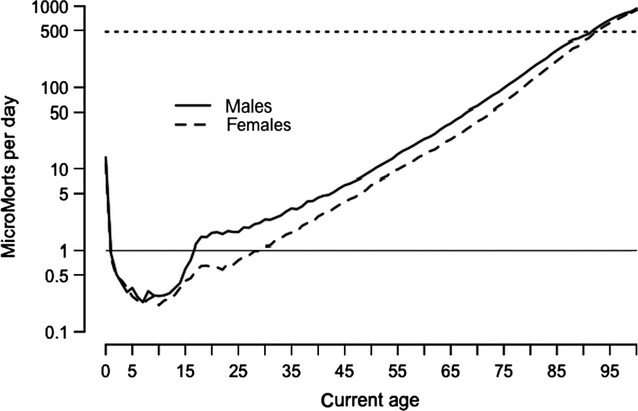
Simply being being alive carries a risk in itself: it is highest on the first day of lift at around 500 micromorts, drops rapidly in childhood and then increases steadily throughout adult life until the 90s, when each day is as risky as that person’s first day.
MicroMorts per day for average person in England and Wales—dashed line shows rate for first day of life. (Spiegelhalter, 2014)
Perhaps unsurprisingly, one UK estimate showed that travelling by motorbike carries the highest risk of death at 9.6km for each MicroMort. Travelling by car is far safer at 400km per MicroMort. But somewhat counterintuitively, walking is not much safer than travelling by motorbike: hitting the pavement results in one MicroMort per 27.2km walked. This can be partly explained by the greater amount of time spent walking and exposed to environmental hazards such as traffic, air pollution, crime and so on.
The concept of micromorts can also be applied to pregnancies and risks to the foetus. The risk per unit due to stillbirth is only about 19 or 3710 micromorts when drinking 5 units/week throughout pregnancy. For low risk women in the UK, planned first birth at home carries an additional 843 (-200 to 2620) micromorts compared with in hospital, and planned vaginal breech birth an additional 5870 (-4400 to 18 500), compared with planned caesarean. By contrast, the risk from the mother eating a serving of unpasteurised cheese, is negligible at 0.00026 micromorts (Hickson et al., 2020).
In a recent analysis published in Acta Obstetricia et Gynecologica Scandinavica, researchers found no link between women’s caffeine consumption and pregnancy or live birth rate after fertility treatments – but alcohol consumption was linked to decreased pregnancy rate after treatments with more than 84g of alcohol a week (approximately 7 standard drinks).
The link held true for their spouses as well: men’s alcohol consumption was associated with decreased live birth rate after fertility treatments in women when weekly consumption was greater than 84g.
The researchers searched the available literature and found a total of 7 studies on caffeine consumption and 9 studies on alcohol consumption were included, with a total of 26 922 women and/or their spouse who underwent fertility treatment.
Compared with those abstaining from alcohol, the chance of achieving a pregnancy after fertility treatment decreased by 7% for women who consumed 84g of alcohol per week, and the chance of partners achieving a live birth decreased by 9% for men who consumed 84g of alcohol per week.
“Couples should be aware that some modifiable lifestyle factors such as drinking habits may affect their fertility treatment outcomes. But how these factors impact the reproductive system still needs more research to elucidate,” said corresponding author Yufeng Li, MD, of Tongji Hospital, in China.
In recent years, researchers have made strides in promoting tissue regeneration in spinal cord injuries (SCI) through implanted neural stem cells or grafts in animal models. Separate efforts have shown that intensive physical rehabilitation can improve function after SCI by promoting greater or new roles for undamaged cells and neural circuits.
University of California San Diego researchers tested whether rehabilitation can pair with pro-regenerative therapies, such as stem cell grafting. They published their findings in in JCI Insight,
The researchers induced a cervical lesion in rats that impaired the animals’ ability to grasp with its forelimbs. The animals were divided into four groups: animals who underwent the lesion alone; animals who received a subsequent grafting of neural stem cells designed to grow and connect with existing nerves; animals who received rehabilitation only; and animals who received both stem cell therapy and rehabilitation.
Rehabilitation therapy for some animals began one month after initial injury, a time point that approximates when most human patients are admitted to SCI rehabilitation centers. Rehabilitation consisted of daily activities that rewarded them with food pellets if they performed grasping skills.
The researchers found that rehabilitation enhanced regeneration of injured corticospinal axons at the lesion site in rats, and that a combination of rehabilitation and grafting produced significant recovery in forelimb grasping when both treatments occurred one month after injury.
“These new findings indicate that rehabilitation plays a critically important role in amplifying functional recovery when combined with a pro-regenerative therapy, such as a neural stem cell transplant,” said first author Paul Lu, PhD, associate adjunct professor of neuroscience at UC San Diego School of Medicine and research health science specialist at the Veterans Administration San Diego Healthcare System.
“Indeed, we found a surprisingly potent benefit of intensive physical rehabilitation when administered as a daily regimen that substantially exceeds what humans are now provided after SCI.”
Senior author Mark H. Tuszynski, MD, PhD, professor of neurosciences and director of the Translational Neuroscience Institute at UC San Diego School of Medicine, and colleagues have long worked to address the complex challenges of repairing SCIs and restoring function.
In 2020, for example, they reported on the observed benefits of neural stem cell grafts in mice and in 2019, described 3D-printed implantable scaffolding that would promote nerve cell growth.
“There is a great unmet need to improve regenerative therapies after SCI,” said Tuszynski. “We hope that our findings point the way to a new potential combination treatment consisting of neural stem cell grafts plus rehabilitation, a strategy that we hope to move to human clinical trials over the next two years.”
The largest ever randomised controlled trial of intensive blood pressure lowering after thrombectomy in ischaemic stroke patients found that it led to deterioration in surrounding brain tissue and higher rates of disability, compared to less intensive treatment.
The results of the ENCHANTED2/MT trial were presented in a late-breaking session at the World Stroke Congress and simultaneously published in The Lancet. The trial was stopped early due to the significance of the findings.
Professor Craig Anderson, Director of Global Brain Health at The George Institute for Global Health, said the rapid emergence of this effect suggested the more aggressive approach was compromising the return of blood flow to the affected area.
“Our study provides a strong indication that this increasingly common treatment strategy should now be avoided in clinical practice,” he said.
Endovascular thrombectomy is an increasingly used non-surgical treatment for ischaemic stroke, in which x-ray guided microcatheters are inserted into the blood clot to dissolve it.
“A potential downside of this now widely used and effective treatment is that the rapid return of blood supply to an area that has been deprived of oxygen for a while can cause tissue damage known as reperfusion injury,” said Professor Anderson.
“This has resulted in a shift in medical practice towards more intensive lowering of blood pressure after clot removal to try and minimise this damage, but without evidence to support the benefits versus potential harms.”
To this end, researchers recruited 816 adults with acute ischaemic stroke who had elevated blood pressure after clot removal from 44 centres in China between July 2020 and March 2022. They had an average age of 67 and just over a third were female.
Of these, 407 were assigned to more-intensive (target < 120mmHg) and 409 to the less-intensive (target 140–180mmHg) systolic blood pressure control, with the target to be achieved within one hour of entering the study and sustained for 72 hours.
Researchers looked at how well the patients in both groups recovered according to a standard measure of disability, ranging from 0–1 for a good outcome without or with symptoms but no disability, scores of 2–5 reflecting increasing disability levels, and 6 being death.
Patients in the more-intensively treated group had significantly worse scores on the scale compared to those allocated to those treated less intensively.
Compared to the less-intensive group, they had more early brain tissue deterioration and major disability at 90 days but there were no significant differences in brain bleeds, mortality, or serious adverse events.
Patients who had their blood pressure more intensively controlled also rated their quality of life as significantly worse due to limitations on their physical abilities resulting from their stroke.
Prof Anderson said that after scouring the medical literature the research team had been unable to find strong enough evidence to recommend the ideal target for blood pressure control after blood clot removal in patients with acute ischaemic stroke.
“While our study has now shown intensive blood pressure control to a systolic target of less than 120mmHg to be harmful, the optimal level of control is yet to be defined,” he said.