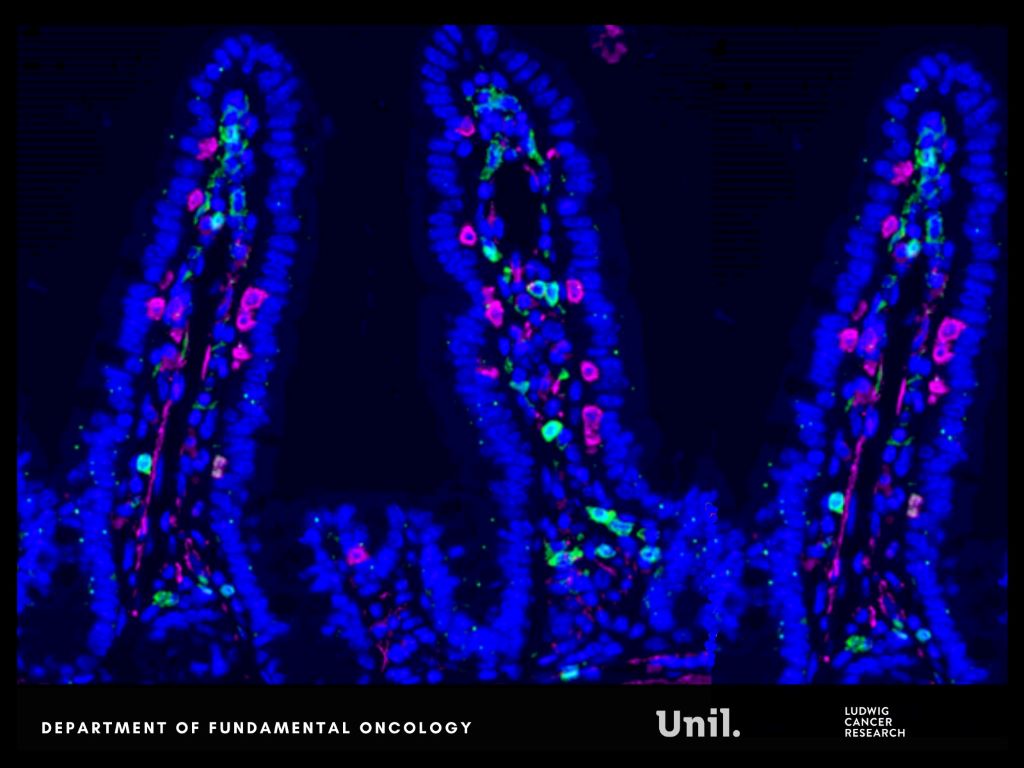
Microscopy image of intestinal lining in mice, shows CD4 (green), CD8 (magenta) and DAPI (blue). Ludivine Bersier 2025
In Nature Communications, researchers from Lusanne University reveal that chemotherapy alters gut microbes and bone marrow immune cell development, unexpectedly reprogramming systemic immunity in ways that help restrict metastatic progression.
Chemotherapy commonly damages the intestinal lining, a well-known side effect. But this injury does not remain confined to the gut. It reshapes nutrient availability for intestinal bacteria, forcing the microbiota to adapt.
The researchers report that chemotherapy-induced damage to the intestinal lining alters nutrient availability for gut bacteria, reshaping the microbiota and increasing the production of indole-3-propionic acid (IPA), a tryptophan-derived microbial metabolite.
Rather than acting locally, IPA functions as a systemic messenger. It travels from the gut to the bone marrow, where it rewires immune cell production. Elevated IPA levels reprogram myelopoiesis, reducing the generation of immunosuppressive monocytes that facilitate immune evasion and metastatic growth.
“We were surprised by how a side effect often seen as collateral damage of chemotherapy can trigger such a structured systemic response. By reshaping the gut microbiota, chemotherapy sets off a cascade of events that rewires immunity and makes the body less permissive to metastasis.” says Ludivine Bersier, first author of the study.
This immune reconfiguration enhances T-cell activity and remodels immune interactions within metastatic niches, particularly in the liver, resulting in a metastasis-refractory state in preclinical models.
Experimental findings are mirrored in patients. Clinical relevance is supported by patient data obtained in collaboration with Dr Thibaud Koessler (Geneva University Hospitals, HUG). In patients with colorectal cancer, higher circulating IPA levels following chemotherapy are associated with reduced monocyte levels, a feature of improved survival outcomes.
“This work shows that the effects of chemotherapy extend far beyond the tumor itself. By uncovering a functional axis linking the gut, the bone marrow and metastatic sites, we highlight systemic mechanisms that could be harnessed to durably limit metastatic progression.” says Tatiana Petrova, corresponding author of the study.
This research was supported by multiple funders, including the Swiss National Science Foundation and Swiss Cancer League. An ISREC Foundation Tandem Grant supported close collaboration between clinical and fundamental research, led at Unil by Professor Tatiana Petrova and Dr Thibaud Koessler at HUG. The project posits that chemotherapy can induce a form of biological “memory”, mediated by gut microbiome–derived metabolites that durably inhibit metastatic growth.
Together, these findings reveal a previously underappreciated gut–bone marrow–liver metastasis axis through which chemotherapy can exert durable systemic effects, opening new avenues to harness microbiota-derived metabolites as adjuvant strategies to limit metastasis.
Long-term use of medications for heartburn and acid reflux, known as proton pump inhibitors, does not appear to increase the risk of stomach cancer, according to a new study published in The BMJ. The results are based on extensive Nordic health data and may provide reassurance to patients who need long-term treatment, according to researchers at Karolinska Institutet.
The possibility that proton pump inhibitors could cause stomach cancer has been discussed since the 1980s. Overall, studies have shown a doubled risk, but the studies have had methodological shortcomings. To investigate the association, taking into account a number of possible sources of error in previous literature in the field, researchers analysed registry data from the five Nordic countries – Denmark, Finland, Iceland, Norway, and Sweden – over a period of up to 26 years.
The study included 17 232 people with stomach cancer and compared them with over 172 000 control subjects matched for age, sex, year, and country. The researchers investigated the use of proton pump inhibitors and another type of acid-suppressing drug, histamine-2 receptor blockers.
To avoid methodological errors, drug use in the last year before diagnosis was excluded, as were patients who had cancer in the upper part of the stomach, where heartburn is a risk factor. The results were also adjusted for factors such as Helicobacter pylori infection, stomach ulcers, smoking, alcohol-related diseases, obesity, diabetes, and certain medications.
By using this methodological approach, the researchers found no association between long-term use of these drugs and the risk of stomach cancer.
“Our results contradict the hypothesis that proton pump inhibitors cause stomach cancer,” says the lead researcher responsible for the study, Professor Jesper Lagergren at the Department of Molecular Medicine and Surgery, Karolinska Institutet. He continues:
“This provides reassurance for patients who need long-term treatment and is important for clinical decisions.”
The researchers emphasise that the study is observational, which means that no definitive conclusions can be drawn about cause and effect. Nor can it be completely ruled out that confounding factors that could not be adjusted for have influenced the results. However, the study design allows for more reliable results than previous research.
People who have ADHD traits at age 10 are more likely than those without such traits to have physical health problems and to report physical health-related disability at age 46, according to a study led by UCL and University of Liverpool researchers.
The researchers say the findings likely reflect the impact of a wide range of risk factors for poor health that are linked to attention deficit hyperactivity disorder (ADHD) and society’s response to people with ADHD across adulthood.
The new JAMA Network Open paper is one of the largest ever studies, with the most years of follow-up, looking at childhood ADHD traits and later health outcomes.
Senior author Professor Joshua Stott (UCL Psychology & Language Sciences) said: “Here we have added to the concerning evidence base that people with ADHD are more likely to experience worse health than average across their lifespan.
“People with ADHD can thrive with the right support, but this is often lacking, both due to a shortage of tailored support services but also because ADHD remains underdiagnosed, particularly in people in midlife and older, with needs unaddressed.”
People with ADHD experience differences in how they focus their attention and/or increased hyperactivity and impulsivity. They can often have high energy and an ability to focus intensely on what interests them, but they may find it difficult to focus on mundane tasks. This can lead to more impulsiveness, restlessness, and differences in planning and time management, which may make it harder to succeed at school and work, leading to longer-term challenges.
ADHD begins in childhood, and while it is increasingly recognised to persist in adults, it is under-treated in adults in the UK compared to in other high-income countries, and support remains under-resourced.
For the study, supported by the Medical Research Foundation, the researchers analysed data from 10 930 participants of the UCL-led 1970 British Cohort Study, a large longitudinal study of people who have been taking part in research from birth to middle age.
ADHD traits were determined based on child behaviour questionnaires completed by parents and teachers when the study participants were 10 years old, regardless of whether they had ever been diagnosed with ADHD.
The researchers found that people with high scores on the index of ADHD traits at age 10 were more likely to have other health conditions by age 46, with 14% higher odds of reporting two or more physical health problems such as migraine, back problems, cancer, epilepsy or diabetes. Among those with high ADHD traits in childhood, 42% had two or more health problems in midlife, compared to 37% of those without high ADHD traits.
People with high ADHD traits at age 10 were also more likely to experience physical health-related disability (reporting having problems with work or other daily activities as a result of their physical health) at age 46.
Their analysis suggests that the poorer health outcomes were partly explained by increased mental health problems, higher BMI and higher smoking rates among people with ADHD. Other studies have found that people with ADHD are also more likely to experience stressful life events and social exclusion, and are less likely to get timely access to screening and medical care.
The researchers found that the link between childhood ADHD traits and physical health-related disability appeared to be stronger among women than men.
Professor Stott added: “All of these potential explanatory factors align with the fact that ADHD makes impulse control more difficult, the need for instant gratification and reward more intense, and is also associated with worse mental health in part due to the social disadvantage people with ADHD face.”
A study published last year by the same research group also found an apparent reduction in life expectancy for adults with diagnosed ADHD, although this was not part of the current study.*
Lead author Dr Amber John, who began the research at UCL before moving to the University of Liverpool, said: “It’s important to note that people with ADHD are a diverse group, with a range of different strengths and experiences, and most will lead long, healthy lives.
“However, many face significant barriers to timely diagnosis and appropriate support. This is important because providing the right support for and meeting the needs of people with ADHD can help to improve their physical and mental health outcomes.
“Additionally, public health strategies should consider the needs of people with ADHD, such as by making screening programmes and ongoing health monitoring more accessible for people with ADHD.”
New research paves way for novel therapies to reverse heart failure
Human heart. Credit: Scientific Animations CC4.0
Pioneering research by experts at the University of Sydney, the Baird Institute and the Royal Prince Alfred Hospital in Sydney has shown that heart muscle cells regrow after a heart attack, opening up the possibility of new regenerative treatments for cardiovascular disease.
Following the publication of the study in Circulation Research, first author Dr Robert Hume, from the Faculty of Medicine and Health and Charles Perkins Centre, and Lead of Translational Research at the Baird Institute for Applied Heart and Lung Research, explained the significance of the finding:
“Until now we’ve thought that, because heart cells die after a heart attack, those areas of the heart were irreparably damaged, leaving the heart less able to pump blood to the body’s organs.
“Our research shows that while the heart is left scarred after a heart attack, it produces new muscle cells, which opens up new possibilities.
“Although this new discovery of regrowing muscle cells is exciting, it isn’t enough to prevent the devastating effects of a heart attack. Therefore, in time, we hope to develop therapies that can amplify the heart’s natural ability to produce new cells and regenerate the heart after an attack.”
Though increased mitosis (a process in which cells divide and reproduce) after a heart attack has been observed in the heart muscles of mice, this is the first time the phenomenon has been demonstrated in humans.
Heart disease in Australia and the world
Cardiovascular disease is the leading cause of death globally, and is responsible for nearly a quarter (24 percent) of all deaths in Australia.
Heart attacks can eliminate a third of the cells in the human heart and, though survival rates have improved dramatically over the last decade thanks to therapeutic advancements, many patients still go on to develop heart failure, which can only be cured with a transplant. With approximately 144 000 heart failure patients in Australia and only 115 heart transplants per year, there is a huge disparity in what these patients need and the treatment that can be offered.
Pioneering techniques made research possible
The study is also the first in the world to use tissue samples taken from living patients during bypass surgery. These “pre-mortem” tissue samples were taken from consenting patients undergoing heart bypass surgery at the Royal Prince Alfred Hospital in Sydney.
The samples were collected from diseased and non-diseased parts of the heart using a method developed by Professor Paul Bannon and Professor Sean Lal, who work jointly at the University of Sydney, Royal Prince Alfred Hospital and The Baird Institute.
New therapies to regenerate the heart
Developing a technique to collect living tissue samples means the research team now has a laboratory model which they hope to use to unlock new treatments to regenerate the human heart.
Professor Sean Lal, senior author of the study from the School of Medical Sciences and heart failure cardiologist at the Royal Prince Alfred hospital, said: “Ultimately, the goal is to use this discovery to make new heart cells that can reverse heart failure.
“Using living human heart tissue models in our work means that we will have more accurate and reliable data to develop new therapies for heart disease.
“Already, our research using these samples has identified several proteins that have previously been shown to be involved in the regeneration of the heart in mice – which is a very exciting prospect to now translate to humans.”
As HIV, TB and other treatments are updated in our public healthcare system, it is critical that healthcare workers and counsellors stay on top of the latest developments. One innovative programme makes use of short lessons delivered over WhatsApp to provide such training.
Over her years working as an information pharmacist at the University of Cape Town’s Medicines Information Centre (MIC), Briony Chisholm noted that many health workers in rural clinics face difficulties accessing training in crucial aspects of their work.
“The lack of easy access to training was in areas where it was really needed, such as the HIV (treatment) guidelines that are constantly being updated,” says Chisholm. “It’s not enough to have training sessions when new guidelines come out; you ideally should be training all the time.”
Drug-drug interactions
At the end of 2019, government introduced new standard first-line HIV treatment that includes an antiretroviral medicine called dolutegravir. As we previously reported, by 2023 around 4.7 million people in South Africa were taking dolutegravir-based treatment.
But the introduction of a new medicine in the public healthcare system, especially at this scale, is rarely straight-forward.
“Dolutegravir is considered as a ‘wonder child’ in ARV treatment, because it provides a high barrier to resistance, is easier to take, and has far fewer side effects than older ARVs. However, it also has interactions with other key drugs, particularly those used for the treatment of TB, diabetes and some anti-epileptic medications,” she says.
Through numerous queries received on the MIC’s National HIV and TB Healthcare Worker Hotline, Chisholm and her colleagues became aware that some healthcare workers were struggling with managing drug interactions. “Some healthcare workers didn’t know about these interactions; others knew about them but not how to deal with them. For example, if a patient is on the TB drug rifampicin, but also needs to take dolutegravir, there’s a need to adjust the dose of dolutegravir. Similarly, adjustments are needed with the diabetes medicine, metformin.”
Chisholm now lives in the Eastern Cape village of Nieu Bethesda. When dolutegravir was introduced, she had just completed her part-time post-graduate Diploma in HIV and TB management through UCT and signed up for her Masters. She and a colleague had, in 2016, done a road trip to about 200 clinics in seven provinces to promote the MIC’s Hotline.
“We saw that most South African healthcare workers are dedicated and keen to learn. You hear all this terrible news about health and corruption, and then you go to these clinics which are ticking along under sometimes difficult conditions, doing amazing work. It’s inspiring!”
A key realisation was the challenges experienced by health workers at these rural clinics to access much-needed training.
“Getting nurses to a central point for training and the need for transport, accommodation and food, as well as having them absent from the clinic for anything between one and five days, is challenging. It’s expensive and involves a great deal of organising,” says Chisholm.
Doing the research
Chisholm then started conducting research on what healthcare workers know about dolutegravir-related drug interactions. Her study, published in 2022, found that about 70 percent of respondents understood that dolutegravir interacts with other drugs, but there were gaps in people’s knowledge of specific interactions and the dosing changes needed to manage those interactions.
The study found that access to guidelines and training were positively associated with knowledge of drug-drug interactions. “There was a clear indication that we needed more accessible training,” Chisholm says.
“The Department of Health offers online training through live webinars, and recordings of these, but they are often one or two hours long. Nurses in busy clinics don’t necessarily have this time to sit through training sessions.”
Testing the efficacy of short training sessions
Chisholm then designed a project to test the efficacy of short training sessions focusing on teaching one or two learning points from the national guidelines in ten to fifteen-minute live lessons using WhatsApp.
“I thought, ‘we’re in a country where not everyone has access to big computer screens, but they all have a cell phone and use WhatsApp – so let’s go as simple as we can’,” she says. “The idea was not to teach the entire set of guidelines but to pick out important parts of them and ensure that if something changes in the guidelines, you get it out to people, quickly.”
Chisholm tested the feasibility of WhatsApp-based microlearning with health workers and counsellors at 50 clinics around Nieu Bethesda. “I ran a range of short case-based lessons on WhatsApp groups and then measured the changes in knowledge and patient care, as well as other factors like uptake, feasibility and accessibility,” she explains.
She found that WhatsApp-based microlearning for healthcare workers is “effective, feasible and well received” and 98 percent of those who participated said they would take part if training sessions were held weekly throughout the year.
While using WhatsApp for medical interactions is not new, Chisholm says a structured syllabus using microlearning for short, punchy sessions is a first.
“This type of learning is equally accessible to a rural clinic as to one in central Hillbrow. We can access people wherever they are. Nobody has to spend money getting anywhere and clinical services are not disrupted. And it doesn’t matter if they’re not in the live session: when they have a moment, they can go into their WhatsApp and read back on the lesson,” she says.
Working with the department of health on 6MMD
Chisholm has been working with the National Department of Health on their Six-Month Multi-Month Dispensing (6MMD) programme. The programme allows people living with HIV who are doing well on treatment and have suppressed viral loads to get a six-month supply of ARVs in one go. This makes life considerably easier for people, since they only need to go to the clinic twice a year; whilst also reducing workloads in the clinics. The programme started in August 2025 and is still being phased in across the country.
“In the pilot phase, the Department of Health did some really good online training and they used our WhatsApp training as an add-on to the longer form training,” says Chisholm.
“We started with one group and ran an eight-week course of 15-minute lessons once a week on WhatsApp. Sessions were case-based and included which patients are eligible for 6MMD, and which patients are not,” she explains. By the end of 2025, around 2 000 healthcare workers had been reached through these sessions.
Lynne Wilkinson, a technical expert with the International AIDS Society which supports the Department of Health on 6MMD, says the microlearning is “a great way to ensure we get to all the clinicians in the country and explain how the 6MMD programme works”.
She adds: “When a new policy comes out, it takes a long time for implementation to be scaled because ground level clinicians aren’t always aware of the changes or don’t have an opportunity to engage with how to implement the changes.”
Daniel Canham, a professional nurse and facility team lead for the NGO, TB HIV Care, at Idutywa Village Community Health Centre in the Eastern Cape, says they’ve found the microlearning sessions for 6MMD very useful. “It’s no secret that the waiting times in clinics are quite extensive, so we are trying to enrol all those qualified for 6MMD as quickly as possible to ease the burden on the clinic,” he says.
“The microlearning on 6MMD has been very helpful. Our staff don’t have to be out of the facility to attend it. They can run their normal activities and attend sessions of ten minutes maximum,” says Canham.
“Our professional nurses joined the WhatsApp microlearning sessions in September last year,” says Faith Maseko, a nurse lead based at Phola Park Clinic in Thokoza in Gauteng who works for the WITS Research Health Institute (RHI). The RHI supports the health department in the management of HIV and employs more than 30 nurses.
“When nurses are trained virtually, some of the information is forgotten, but when you’re on WhatsApp, you can go back and access the information that was shared. The scenarios provided are very useful. If you see a patient, with a similar scenario you can go back and see what was discussed and apply it to your own situation,” she says.
Department of Health backing
Foster Mohale, spokesperson for the National Department of Health, says the WhatsApp-based microlearning has been “an effective low-cost, high-reach supplement to formal 6MMD training”.
He adds: “Training gaps translate directly into service gaps, affecting quality, retention, and progress toward epidemic control. Microlearning addresses this risk by enabling continuous, bite-sized reinforcement of policy and implementation guidance, rather than relying solely on once-off training events. This approach supports frontline healthcare workers in applying 6MMD consistently under real-world service pressures.”
Mohale says evidence from the department’s broader capacitation strategy shows that lifelong, continuous learning, rather than episodic training, is essential for resilient health systems.
“WhatsApp microlearning aligns with this principle by supporting rapid dissemination of updates, peer learning, and sustained mentorship. When integrated with structured models and aligned to national guidelines, it can be effectively applied across HIV, TB, maternal and child health, non-communicable diseases, and health systems strengthening more broadly,” he says.
Red Blood Cell Infected with Malaria Parasites Colourised scanning electron micrograph of red blood cell infected with malaria parasites (teal). The small bumps on the infected cell show how the parasite remodels its host cell by forming protrusions called ‘knobs’ on the surface, enabling it to avoid destruction and cause inflammation. Uninfected cells (red) have smoother surfaces. Credit: NIAID
A new clinical trial led by QIMR Berghofer, in collaboration with University of Sunshine Coast Clinical Trials Network has found a medication currently used for some blood disorders could help the body fight malaria more effectively.
The findings mean the drug, ruxolitinib, could potentially be used alongside standard treatment to boost recovery and strengthen people’s immune systems against future infections.
Malaria kills more than 600 000 people each year and three quarters of those deaths are in children under the age of five.
Current treatments for malaria work by killing the parasite that causes most malaria deaths, Plasmodium falciparum. However, even with these treatments, fatality rates from severe malaria remain high.
Furthermore, while patients develop some immunity after infection, this protection is often incomplete, leaving many vulnerable to reinfection.
“While antimalarial treatments are effective at killing the parasite, they don’t directly address the inflammation that contributes to severe illness and death. These findings suggest that we may be able to improve clinical outcomes by targeting the host inflammatory response as well as the parasite itself,” she said.
The research, published in Science Translational Medicine, looked at how the immune system responds to malaria via the body’s ‘early warning system’ known as type 1 interferon signalling.
To do this, researchers enrolled 20 healthy adult volunteers who had never been exposed to malaria. Participants were deliberately infected with Plasmodium falciparum under closely monitored conditions. Eight days later, all participants received standard malaria treatment (artemether-lumefantrine), while 11 were also given ruxolitinib. Three months later, participants were re-infected with malaria to test how their immune systems responded to a second infection.
The research revealed ruxolitinib was safe and well-tolerated, compared with the placebo group, and participants who received ruxolitinib showed a lower inflammatory response, and favourable changes in markers linked to disease severity.
QIMR Berghofer’s Program Director of Infection and Inflammation Professor Christian Engwerda says the results are encouraging.
“One of the biggest challenges in efforts to eliminate malaria is the limited efficacy and duration of protection provided by current vaccines. By boosting the immune system without causing detrimental inflammation with drugs like ruxolitinib, we may be able to overcome these challenges,” he said.
The researchers say it’s important to note that the study was conducted in healthy volunteers who did not live in malaria-endemic regions. Further studies in malaria-endemic regions will be needed to determine whether these findings translate into improved outcomes for patients most affected by the disease.
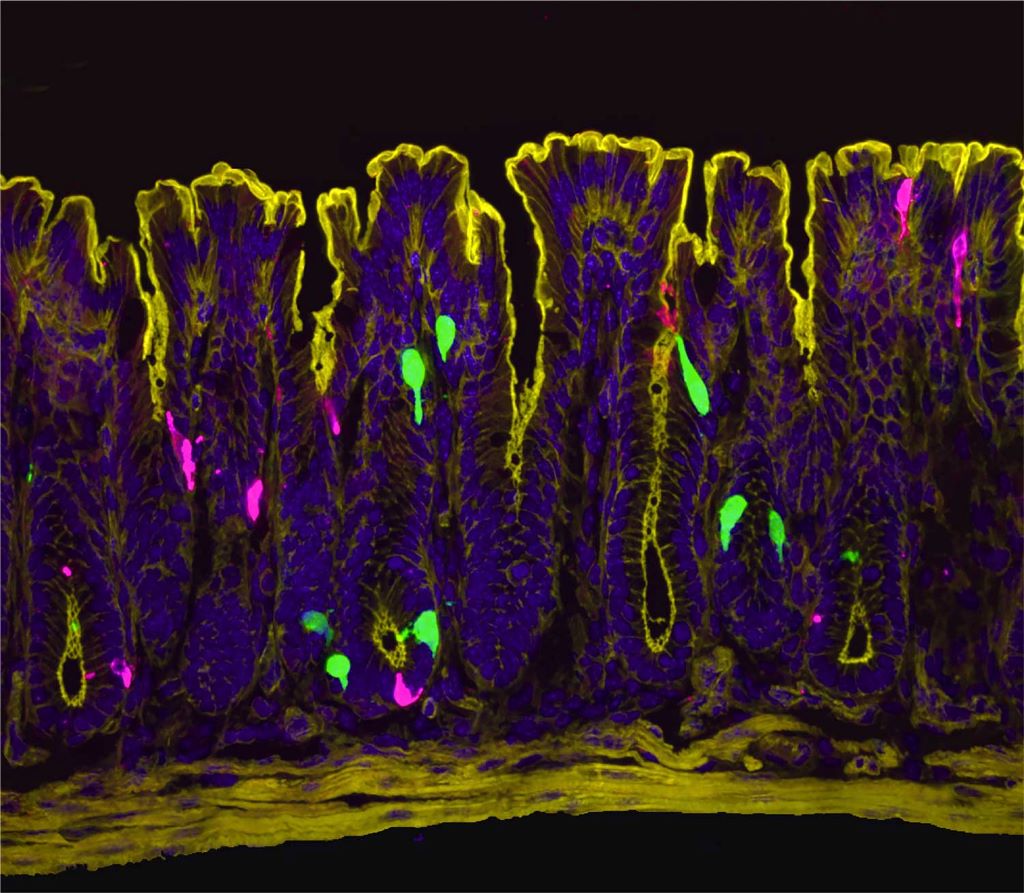
UCSF researchers discover that oestrogen can turn on pain signals associated with conditions like irritable bowel syndrome.
A zoomed in image of the lining of the colon. Cells that produce the hormone PYY (peptide YY) are in green. Cells that produce the neurotransmitter serotonin are in magenta. PYY triggers the release of serotonin, which activates pain-sensing nerve fibers. Image by Archana Venkataraman/UCSF
Women are dramatically more likely than men to suffer from irritable bowel syndrome (IBS), a chronic condition causing abdominal pain, bloating, and digestive discomfort. Now, scientists at UC San Francisco have discovered why.
Oestrogen, the researchers report in Science, activates previously unknown pathways in the colon that can trigger pain and make the female gut more sensitive to certain foods and their breakdown products. When male mice were given oestrogen to mimic the levels found in females, their gut pain sensitivity increased to match that of females.
The findings not only explain the female predominance in gut pain disorders but also point to potential new ways to treat the conditions.
“Instead of just saying young women suffer from IBS, we wanted rigorous science explaining why,” said Holly Ingraham, PhD, professor UCSF and co-senior author of the study. “We’ve answered that question, and in the process identified new potential drug targets.”
The research also suggests why low-FODMAP diets – which eliminate certain fermentable foods, such as onions, garlic, honey, wheat, and beans – help some IBS patients, and why women’s gut symptoms often fluctuate with their menstrual cycles.
“We knew the gut has a sophisticated pain-sensing system, but this study reveals how hormones can dial that sensitivity up by tapping into this system through an interesting and potent cellular connection,” said co-senior author David Julius, PhD. Julius won the 2021 Nobel Prize for Physiology or Medicine for his work on pain sensation.
Search for oestrogen
Previous research had hinted that oestrogen was to blame for higher rates of IBS in females, but not why. To understand how oestrogen might be involved, Ingraham’s and Julius’s teams first needed to see exactly where the hormone was working in the gut.
“At the time I started this project, we didn’t know where and how oestrogen signalling is set up in the female intestine,” said Archana Venkataraman, PhD, a postdoc in Ingraham’s lab and co-first author of the research. “So, our initial step was to visualise the oestrogen receptor along the length of the female gut.”
The team expected to see oestrogen receptors in enterochromaffin (EC) cells, which were already known to send pain signals from the gut to the spinal cord. Instead, they got a surprise: oestrogen receptors were clustered in the lower part of the colon and in a different cell type known as L-cells.
The scientists pieced together a complex chain reaction that occurs when oestrogen binds to the L-cells. First, oestrogen causes L-cells to release a hormone called PYY (peptide YY). PYY then acts on neighbouring EC cells, triggering them to release the neurotransmitter serotonin, which activates pain-sensing nerve fibres. In female mice, removing the ovaries or blocking oestrogen, serotonin, or PYY dramatically reduced the high gut pain observed in females.
For decades, scientists believed PYY primarily suppressed appetite – drug companies even tried developing it as a weight-loss medication. But those clinical trials failed due to a troubling side effect that was never fully explained; participants experienced severe gut distress. The new findings mesh with this observation and suggest a completely new role for PYY.
“PYY had never been directly described as a pain signal in the past,” said co-first author Eric Figueroa, PhD, a postdoc in Julius’ lab. “Establishing this new role for PYY in gut pain reframes our thinking about this hormone and its local effects in the colon.”
This video shows what happens to the enterochromaffin (EC) cells in the colon when they are treated with PYY. Upon PYY treatment, calcium activity increases in the EC cell, causing it to fluoresce more brightly as it releases serotonin that is detected by nearby pain-sensing nerve fibres. Video by Eric Figueroa/UCSF
A link between IBS and diet
Increased PYY wasn’t the only way that L-cells responded to oestrogen. Levels of another molecule, called Olfr78, also went up in response to the hormone. Olfr78 detects short-chain fatty acids – metabolites produced when gut bacteria digest certain foods. With more Olfr78 receptors, L-cells become hypersensitive to these fatty acids and are more easily triggered to become active, releasing more PYY.
“It means that oestrogen is really leading to this double hit,” said Venkataraman. “First it’s increasing the baseline sensitivity of the gut by increasing PYY, and then it’s also making L-cells more sensitive to these metabolites that are floating around in the colon.”
The observation may explain why low-FODMAP diets help some IBS patients. FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) are carbohydrates that gut bacteria ferment into those same fatty acids sensed by Olfr78. By eating fewer FODMAPs, patients may be preventing the activation of Olfr78, and, in turn, keeping L-cells from churning out more of the pain signalling PYY.
While men have this same cellular pathway, their lower oestrogen levels keep it relatively quiet. However, the pathway could engage in men taking androgen-blocking medications, which block the effects of testosterone and can elevate oestrogen in some cases, potentially leading to digestive side-effects.
The new work suggests potential ways to treat IBS in women and men alike.
“Even for patients who see success with a low-FODMAP diet, it’s nearly impossible to stick to long term,” Ingraham said. “But the pathways we’ve identified here might be leveraged as new drug targets.”
The researchers are now studying how such drugs might work, as well as asking questions about what other hormones, such as progesterone, might play a role in gut sensitivity and how pregnancy, lactation, and normal menstrual cycles affect intestinal function.
Super agers were 68% less likely to harbour the gene nobody wants, APOE-ε4, compared to individuals with AD dementia in the same 80+ age group.
Photo by Ravi Patel on Unsplash
A comparatively large study reported Jan. 16 in Alzheimer’s & Dementia, The Journal of the Alzheimer’s Association, led by researchers at Vanderbilt Health, measures the frequency ofAPOE-ε4 and APOE-ε2 in so-called super agers — people ages 80 or older whose cognitive function is comparable to people 20 or 30 years younger.
The gene variant posing the greatest genetic risk of late-onset Alzheimer’s disease (AD) is called APOE-ε4. A different variant of the same gene, APOE-ε2, is thought to confer protection against AD.
Super agers were 68% less likely to harbour the gene nobody wants, APOE-ε4, compared to individuals with AD dementia in the same 80+ age group.
Most notably, super agers were 19% less likely to harbour APOE-ε4 than were cognitively normal participants in the same age group.
“This was our most striking finding – although all adults who reach the age of 80 without receiving a diagnosis of clinical dementia exhibit exceptional aging, our study suggests that the super-ager phenotype can be used to identify a particularly exceptional group of oldest-old adults with a reduced genetic risk for Alzheimer’s disease,” said Leslie Gaynor, PhD, assistant professor of Medicine in the Division of Geriatric Medicine, who led the study with Alaina Durant, BS, statistical genetic analyst in the Vanderbilt Memory and Alzheimer’s Center.
Super agers were also found for the first time to have higher frequency of the variant you’d want, APOE-ε2: They were 28% more likely to carry APOE-ε2 than were cognitively normal controls ages 80+, and 103% more likely to carry the variant than were participants with AD dementia age 80 or older.
The observational study, which includes the largest sample of super agers to date, uses data from the Alzheimer’s Disease Sequencing Project Phenotype Harmonization Consortium, led by another member of the study team, Timothy Hohman, PhD, professor of Neurology. The study included 18,080 participants from eight national aging cohorts.
Super-ager status was defined in part as people ages 80+ whose memory performance was above the average scored among cognitively normal participants ages 50 to 64. The study included multiple race/ethnicity groups, including 1412 non-Hispanic white super agers, 211 non-Hispanic Black super agers, 8829 participants with AD dementia, and 7,628 cognitively normal controls. APOE-ε4 frequency worldwide is 13.7%; in the study it was 43.9%.
“With interest in super agers growing,” Gaynor said, “our findings notably encourage the view that the super-ager phenotype will prove useful in the continued search for mechanisms conferring resilience to AD.
“This is by far the largest study to date to identify differences in APOE-ε4 allele frequency based on super-ager status, and the first study to find a relationship between APOE-ε2 allele frequency and super-ager status. We would expect these findings to lend continued interest to questions of how these variants may influence development of clinical dementia due to Alzheimer’s disease, as well as to the super-ager phenotype more generally.”
When Americans begin taking appetite-suppressing drugs like semaglutide, the changes extend well beyond the bathroom scale. According to new research, the medications are associated with meaningful reductions in how much households spend on food, both at the grocery store and at restaurants.
The study, published December 18 in the Journal of Marketing Research, links survey data on GLP-1 receptor agonist use with detailed transaction records from tens of thousands of U.S. households. The result is one of the most comprehensive looks yet at how GLP-1 adoption is associated with changes in everyday food purchasing in the real world.
The headline finding is striking: Within six months of starting a GLP-1 medication, households reduce grocery spending by an average of 5.3%. Among higher-income households, the drop is even steeper, at more than 8%. Spending at fast-food restaurants, coffee shops and other limited-service eateries falls by about 8%.
Among households who continue using the medication, lower food spending persists at least a year, though the magnitude of the reduction becomes smaller over time, say co-authors, assistant professor Sylvia Hristakeva and professor Jura Liaukonyte, both in the Charles H. Dyson School of Applied Economics and Management in the Cornell SC Johnson College of Business.
“The data show clear changes in food spending following adoption,” Hristakeva said. “After discontinuation, the effects become smaller and harder to distinguish from pre-adoption spending patterns.”
Unlike previous studies that relied on self-reported eating habits, the new analysis draws on purchase data collected by Numerator, a market research firm that tracks grocery and restaurant transactions for a nationally representative panel of about 150 000 households. The researchers matched those records with repeated surveys asking whether household members were taking GLP-1 drugs, when they started and why.
That combination allowed the team to compare adopters with similar households that did not use the drugs, isolating changes that occurred after medication began.
The reductions were not evenly distributed across the grocery store.
Ultra-processed, calorie-dense foods – the kinds most closely associated with cravings – saw the sharpest declines. Spending on savory snacks dropped by about 10%, with similarly large decreases in sweets, baked goods and cookies. Even staples like bread, meat and eggs declined.
Only a handful of categories showed increases. Yogurt rose the most, followed by fresh fruit, nutrition bars and meat snacks.
“The main pattern is a reduction in overall food purchases. Only a small number of categories show increases, and those increases are modest relative to the overall decline,” Hristakeva said.
The effects extended beyond the supermarket. Spending at limited-service restaurants such as fast-food chains and coffee shops fell sharply as well.
The study also sheds light on who is taking GLP-1 medications. The share of U.S. households reporting at least one user rose from about 11% in late 2023 to more than 16% by mid-2024. Weight-loss users skew younger and wealthier, while those taking the drugs for diabetes are older and more evenly distributed across income groups.
Notably, about one-third of users stopped taking the medication during the study period. When they did, their food spending reverted to pre-adoption levels – and their grocery baskets became slightly less healthy than before they started, driven in part by increased spending on categories such as candy and chocolate.
That movement underscores an important limitation, the authors caution. The study cannot fully separate the biological effects of the drugs from other lifestyle changes users may make at the same time. However, evidence from clinical trials, combined with the observed reversion in spending after discontinuation, suggests appetite suppression is likely a key mechanism behind the spending changes.
The findings carry implications far beyond individual households.
For food manufacturers, restaurants and retailers, widespread GLP-1 adoption could mean long-term shifts in demand, particularly for snack foods and fast food. Package sizes, product formulations and marketing strategies may need to change. For policymakers and public-health experts, the results add context to ongoing debates about the role of medical treatments in shaping dietary behavior – and whether biologically driven appetite changes succeed where taxes and labels have struggled.
“At current adoption rates, even relatively modest changes at the household level can have meaningful aggregate effects,” Hristakeva said. “Understanding these demand shifts is therefore important for assessing food markets and consumer spending.”
New research reveals that activating the brain’s reward system through positive anticipation strengthens the immune response and increases antibody production
Can positive anticipation that activates the brain’s reward system strengthen the body’s immune defences? A new study by Tel Aviv University, the Technion, and Tel Aviv Medical Center (Ichilov), published in the prestigious journal Nature Medicine, provides the first evidence in humans that brain activity associated with the expectation of reward has a measurable effect on the body’s response to a specific vaccine.
Eighty-five healthy volunteers participated in the experiment. Some underwent special brain training using fMRI neurofeedback technology – a method that enables individuals to learn, in real time, to regulate activity in specific brain regions through reinforcing learning. The aim of the brain training was to increase activity in a key region of the brain’s reward system including the Ventral Tegmental Area (VTA), which is responsible for dopamine release in the context of mental activity related to the expectation of positive outcomes and motivation to obtain rewards. Participants were instructed to modulate their brain activity using various mental strategies (eg, thoughts, feelings, memories) while monitoring positive feedback about the strategy that was successful in regulating their brain.
From Brain Activation to Antibodies
Immediately after completing the brain training, all participants received a hepatitis B vaccine. The researchers then tracked the immune response through a series of blood tests, measuring levels of specific antibodies produced following the vaccination.
The results showed that participants who succeeded in significantly increasing activity in the brain’s reward region also demonstrated a greater increase in antibody levels after vaccination. The association was specific to the VTA and was not observed in other brain regions used for control purposes (such as the hippocampus), nor in other reward-system areas linked to different reward-related experiences such as pleasure and satisfaction. In other words, the effect was both anatomically and mentally specific.
The Role of Positive Anticipation
Furthermore, an in-depth analysis of the mental strategies participants used during training of the VTA (and not other regions) revealed that those who focused on positive anticipation, such as belief in a good outcome, or the expectation of something positive about to happen, were able to maintain higher VTA brain activity over time, which was also associated with a better immune response. In other words, the researchers identified a link between reward-system brain activity, a mental state of positive anticipation, and the body’s response to an immune challenge.
According to the research team, this is not “positive thinking” in the popular sense or a New Age slogan, but a measurable neurobiological mechanism – related, among other things, to the well-known placebo effect in medicine (a therapeutic response beyond a specific medical intervention). “We show that mental states have a clear brain signature, and that this signature can influence physiological systems such as the immune system,” explain the researchers.
While the study does not propose a substitute for vaccines or medical treatment, it opens the door to new, noninvasive approaches that may one day strengthen immune responses, improve the effectiveness of medical treatments, and even contribute to fields such as immunotherapy and the treatment of chronic immune pathologies. The researchers note that the study’s findings underscore a broader message: the mind–body connection is not merely a theoretical concept, but a real biological process that can be measured, trained, and potentially harnessed to promote better health.
Implications for Medicine and Health
The research team adds that the findings highlight the potential inherent in integrating neuroscience, psychology, and medicine. “Our study shows that the brain is not only a system that responds to the body’s state of health, but also an active player that influences it,” say the researchers. “The ability to consciously activate brain mechanisms associated with positive anticipation opens a new avenue for research and future treatments – as a complement to existing medicine, not as a replacement. In the future, it may be possible to develop simple, noninvasive tools to help strengthen immune responses and enhance the effectiveness of medical treatments by relying on the brain’s natural capacity to influence the body. However, it is important to emphasise that activation of the reward system and its effect on immune response vary between individuals. Therefore, this approach cannot replace existing medical treatments, but may well serve as an additional supportive component.”