Alcohol withdrawal syndrome (AWS) is a potentially life-threatening condition that may complicate patients’ recovery after surgery.
Previous studies have estimated that up to 50% of hospitalised patients with AUD will develop some degree of AWS. Up to 7% of these patients may progress to severe withdrawal, including delirium tremens (DT) that can range in severity from irritability and confusion to tremors, nausea, vomiting and seizures.
Of those patients, 16 504 (0.5%) were diagnosed with AWS, including 6591 (0.2%) with DT.
“We found that alcohol withdrawal syndrome is linked with poorer surgical outcomes, extended hospitalisations and increased costs. These findings underscore the need for standardised perioperative screening and targeted management strategies to reduce these risks,” said study lead author Timothy Pawlik, MD, PhD, professor and chair of Ohio State’s Department of Surgery.
Patients with AWS were generally younger, male and more likely to have Medicaid, according to Pawlik, who holds the Urban Meyer III and Shelley Meyer Chair for Cancer Research at The Ohio State University College of Medicine.
AWS raises the risk of postoperative complications, especially respiratory failure and sepsis. The study found that patients with AWS had longer hospital stays (median 11 vs 6 days) and higher costs ($44 300 vs $28 800).
AWS was associated with a $10 030 higher adjusted hospitalisation cost per patient undergoing surgical care, contributing to an overall excess cost of $165.6 million, said study first author Azza Sarfraz, MBBS, a surgical oncology fellow at Ohio State.
“The lack of standard screening delays early detection and intervention,” Pawlik said. “Developing strategies for early identification, inpatient withdrawal management, and perioperative risk stratification may improve surgical outcomes, lower healthcare costs, and enhance patient care.”
A procedure that can be performed under mild sedation in less than two hours by an interventional radiologist relieves chronic knee pain caused by osteoarthritis, an NYU Langone Health study shows.
As they gradually break down, knee joints in people with osteoarthritis are known to become inflamed, which triggers the growth of small blood vessels (angiogenesis) and increased blood flow to joints. The study procedure, called genicular artery embolisation, kept this abnormal blood flow from ferrying in immune cells that cause the inflammation and related pain.
For the new study, the researchers delivered chemical beads (biocompatible hydrogels) through an image-guided plastic tube to block blood flow in any of a half dozen arteries feeding the synovium lining in the knee. More than 60% of the 25 men and women who had the procedure at its facilities in Manhattan experienced significant improvements one year later.
“Our study shows that genicular artery embolisation is a safe and effective, minimally invasive treatment for those with moderate to severe symptomatic knee pain tied to osteoarthritis,” said study co-investigator and interventional radiologist Ryan M. Hickey, MD. “This work also provides evidence that genicular artery embolisation is offering more than just pain relief and could be modifying the disease process itself.”
“This procedure is particularly suited to those patients who are either not yet ready for knee replacement surgery or for whom surgery is not an option because of age or other risk factors, such as obesity, uncontrolled diabetes or heart disease, or smoking,” added Dr Hickey.
He says there is urgent need for alternative, less-invasive treatments for osteoarthritis. An estimated 24 million cases of osteoarthritis in a knee are diagnosed each year in the United States, a number he expects only to grow with the aging population.
Among the study’s other key results: significant, one-year postsurgical declines (on average 12%) in blood levels of vascular endothelial growth factor (VEGF), a protein that is needed to stimulate the formation of new blood vessels. Past research has also linked VEGF to other structural changes in the knee from osteoarthritis. Another protein biomarker, interleukin 1 receptor agonist (IL-1Ra), showed a similar decrease (15%). IL-1Ra is known for its role in countering inflammation. Tests of a half dozen other immune molecules involved in inflammation were inconclusive.
“Our research suggests that declines in vascular endothelial growth factor could serve as a valuable biomarker or chemical trace for determining success with genicular artery embolisation, offering a much-needed objective benchmark by which to measure its effectiveness,” said study principal investigator and lead author Bedros Taslakian, MD, MA.
“Our study findings also indicate that genicular artery embolisation may, if further larger clinical trials prove successful, slow down the progression of osteoarthritis by observing significant decreases in signalling proteins, specifically vascular endothelial growth factor and interleukin 1 receptor agonist, one year after the procedure,” said Dr Taslakian.
The improvements seen in the 25 patients in the current study were captured by standard patient survey scores for knee pain, stiffness, and the ability to bend, stand up, or walk up and down stairs freely. While subjective surveys are useful in monitoring disease progression, Dr Hickey says, independent blood tests like the NGF measure are more accurate and convenient for patients for tracking small declines or improvements over time.
The NYU Langone team has plans to further investigate precisely how embolisation alleviates inflammation and leads to pain relief.
Dr Hickey also says that more research is needed to establish how long the procedure’s benefits last and which osteoarthritis patients are most likely to benefit.
All study volunteers were diagnosed with moderate to severe osteoarthritis in the knee that had been unresponsive to first-line therapy. This includes knee injections of corticosteroids to reduce inflammation; fluid aspiration (arthrocentesis) to remove excess fluid from the joint; and injections of platelet-rich plasma to repair damaged tissue, as well as physiotherapy. Study participant ages ranged from 50 years old to 78 years old, with all having their embolisation procedures performed between January 2021 and January 2023.
As part of the procedure, interventional radiologists accessed each patient’s arteries through a small incision in the thigh, using video X-ray to guide the catheter to the precise knee artery selected earlier for embolisation. Study participants were then monitored during routine checkups for at least one year and across two dozen measures of pain, knee stiffness, and their ability to move about. Patients needed to achieve a four-point difference on a scale of 20 points to establish a clinically significant reduction in pain. Side effects from the procedure, the researchers say, were minimal and limited to dark skin blemishes on the knee and mild pain near the incision site.
Researchers at Children’s Hospital of Philadelphia (CHOP), along with several academic partners, announced the primary results of the Pediatric KIDney Stone (PKIDS) trial, the largest comparative effectiveness study of surgical interventions for children and adolescents with kidney stones. The CHOP-led PKIDS trial, with two published studies, marks a significant breakthrough by offering stronger evidence for treating stones of varying sizes, including new information on patient experiences after surgery, thus reducing uncertainty and empowering informed decision-making for patients, caregivers, and physicians.
Kidney stones were once largely a disease that affected adults. However, kidney stones in children have been on the rise in recent decades, doubling the likelihood that a child will develop a kidney stone. As a result, CHOP founded the PKIDS Care Improvement Network in 2019, which now includes 31 sites in the United States and Canada.
Ureteroscopy (an endoscopic outpatient procedure), shockwave lithotripsy (a noninvasive outpatient procedure) and percutaneous nephrolithotomy (a minimally invasive surgery with a short hospital stays) are the procedures used to treat children and adults with kidney stones. Most children and adolescents with kidney and ureteral stones are treated with ureteroscopy despite uncertainty of which procedure is more effective and their impact on patients’ lives. As pioneers in urology, CHOP leaders aimed to enhance pediatric patient and caregiver decision-making for kidney stone surgeries while enabling urologists to adopt techniques for optimal outcomes, including patient-selected experiences.
In the first study in JAMA Network Open, Tasian and his team enrolled 1142 patients aged 8 to 21 with kidney and/or ureteral stones between 2020 and 2023 at all 31 sites in the United States and Canada. Researchers evaluated ureteroscopy against shockwave lithotripsy and found that shockwave lithotripsy was associated with less pain and fewer urinary symptoms compared with those who had ureteroscopy. No meaningful differences were detected in stone-free rates for the procedures.
In the other CHOP-led study in JAMA Network Open, Jonathan S. Ellison, MD, an Associate Professor of Urology at the Medical College of Wisconsin and Pediatric Urologist at Children’s Wisconsin, and the PKIDS team compared percutaneous nephrolithotomy (PCNL) and ureteroscopy. That study found that for children with larger stones, PCNL not only cleared more stones effectively but also led to a better overall recovery experience than ureteroscopy.
Overall, the authors emphasised the post-surgery experiences of children, noting that quality of life factors, such as the loss of school time for children and work time for caregivers, are crucial in determining effective treatment options. While the authors are planning further research, they also hope these findings will lead to immediate improvements for families.
“The PKIDS trial demonstrated that ureteroscopy and shockwave lithotripsy remove stones equally well and that patients having shockwave lithotripsy recover more quickly after surgery with less pain and fewer urinary symptoms. Our findings provide new information that allow for tailored approaches to kidney stone treatment for children and their families,” said Gregory E. Tasian, MD, MSc, MSCE, Director of the PKIDS network and an attending pediatric urologist in the Division of Urology at Children’s Hospital of Philadelphia. “Although future clinical trials are important, we hope that clinical practice guidelines will consider outcomes that matter to patients.”
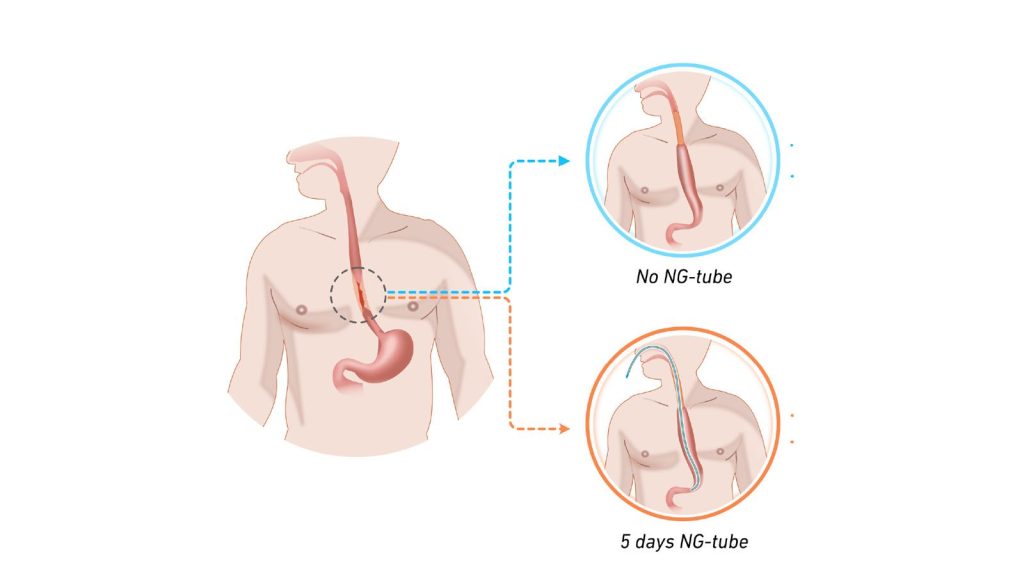
To the researchers’ surprise, it was not without risk to omit the tube after this surgery. Illustration: Jakob Hedberg
In the largest Nordic study to date concerning oesophageal cancer surgery, the researchers found clear evidence that decompression with a nasogastric tube is associated with less serious complications. Their results challenge a trend of declining use of the nasogastric tube after major surgical procedures. The study was led from Uppsala University and has now been published in Lancet Regional Health Europe.
A number of small studies had previously suggested that it is safe to abandon the tradition of leaving in a decompressing – but for many patients unpleasant – nasogastric tube after surgery to remove oesophageal cancer (gullet cancer). The tube is plastic and runs from the nose down to the stomach, and its use in this particular context is to relieve and reduce pressure in this newly operated area. When the question was discussed in a Nordic research collaboration, it was concluded that these smaller studies lacked sufficient statistical power to justify a change in care. Subsequently, a randomised trial was carried out at 12 university hospitals across Sweden, Norway, Denmark and Finland, where patients were randomised to have or not have a decompressing nasogastric tube in their oesophagus following this type of surgery.
Patients without the tube experienced leakage
To the researchers’ surprise, it was not without risk to omit the tube after this surgery, as more patients without the tube experienced leakage in the anastomosis created during the operation. Leakage must be treated immediately, often with interventions under general anaesthesia, resulting in suffering for the patient and a longer length of hospital stay.
Although no differences in survival rates or other complications were found, this new knowledge may help to reduce suffering for patients in the future.
“Oesophageal cancer is an uncommon form of cancer, with only about 200 operations of this type being performed per year in Sweden. National and international cooperation is therefore absolutely necessary in order to conduct sufficiently large trials to answer the research questions we have. The fact that in just over two years, almost 450 patients have been recruited for the trial surpassed our expectations and represents a great success for this network,” says Jakob Hedberg, surgical oncologist, associate professor at Uppsala University and consultant surgeon at Uppsala University Hospital who is also principal investigator for the study.
“Strong interest has been shown at international conferences where our preliminary results have been presented, and the principle of building surgical care on solid evidence has allowed us to provide the best care to our patients. Another important effect of this successful collaboration is that we can build more clinical trials within the Nordic network which has now been consolidated. In fact, the next clinical trial is already under development,” says Jakob Hedberg.
In a study conducted in Uganda and published in JAMA Surgery, researchers from Karolinska Institutet evaluated a new surgical method for treating groin hernias in women. The method could become an alternative in resource-limited settings where laparoscopic techniques are not generally available.
Groin hernia repair is the most common general surgical procedure in the world. Groin hernias are more common in men, but women are more likely to experience complications due to this condition.
Many women in low- and middle-income countries who need surgery for groin hernias lack access to laparoscopy (keyhole surgery). To evaluate a new method using open surgery, the researchers conducted a randomised clinical trial at two publicly funded hospitals in Uganda. The study included 200 women who underwent groin hernia surgery and were followed up after two weeks and after one year.
There are two main types of groin hernias, called inguinal and femoral hernias. The evaluation showed that the new surgical method was effective for both femoral and inguinal groin hernias.
Its effectiveness for both types is particularly important as the study also showed that nearly 45% of the women had femoral hernias, which carry a higher risk of complications.
“The fact that so many of the women had femoral hernias was unexpected and highlights the need to develop effective, safe and accessible methods,” says Alphonsus Matovu, PhD at the Department of Molecular Medicine and Surgery, Karolinska Institutet and first author of the article.
Millions of women affected
The results are promising as the new method could be developed into a viable alternative where access to advanced laparoscopic surgery is limited.
“Women with groin hernias can suffer serious and even fatal complications and therefore need access to effective surgical methods,” says Jenny Löfgren, docent at the same department and last author of the article. “The new method could become a valuable tool to improve care for millions of women”.
The method needs further evaluation, and the researchers will also follow up with the study participants five years after surgery to ensure long-term results. To improve treatment, the new method will also be compared with other surgical methods, both open and laparoscopic.
Research from ICES, Sunnybrook Research Institute and U of T’s Temerty Faculty of Medicine highlights the potential of using team design to improve patient outcomes
Photo by Jafar Ahmed on Unsplash
The odds of patient complications following high-risk surgeries is lower when the surgeon and anaesthesiologists have prior experience working together, according to a new study by researchers at ICES, Sunnybrook Research Institute and the University of Toronto.
The findings come from an analysis of data from hundreds of thousands of high-risk surgeries in Ontario over a 10-year period, along with information on the surgeon and anesthesiologist for each procedure and how often the pair had worked together in the previous four years.
The study, which was recently published in JAMA Surgery, highlights the potential of using team design to improve patient outcomes.
“Team design is used in a lot of other fields like business and sports, but it’s overlooked in health care,” says lead author Julie Hallet, a scientist at Sunnybrook Research Institute and an associate professor of surgery at U of T’s Temerty Faculty of Medicine. “Health care is one of the only areas where we expect people who have never worked together – who sometime have never met before – to perform at peak levels in the most stressful circumstances.”
As a surgeon, Hallet knows first-hand how the environment in an operating room can change depending on team members’ familiarity with each other. It’s something that she and her colleagues have all observed but until recently, lacked the data to describe.
To study this question, Hallet and colleagues analysed population-based health-care data from 711 005 high-risk elective surgeries performed in Ontario between 2009 and 2019, and corresponding information on surgeon-anaesthesiologist teams.
They found that for surgeries related to the gastrointestinal tract, spine and gynaecological cancers, there was an association between surgeon-anaesthesiologist familiarity and the odds of severe complications in the 90 days after surgery – for each additional procedure performed by the same surgeon-anaesthesiologist pair, the likelihood of experiencing a severe complication decreased by three to eight per cent.
“Those are meaningful differences because severe post-operative complications can lead to additional surgeries, ICU stays or even death,” says Hallet.
The researchers also noted that for most procedures, the average surgeon-anaesthesiologist pair were in the operating room together three times a year or less. The exceptions were orthopaedic and cardiac surgery, where surgeons teamed up with the same anaesthesiologist for an average of eight and nine procedures each year, respectively.
These procedures had greater team stability because anaesthesiologists require specialized training to participate in cardiac surgeries and orthopaedic surgeries are often done at dedicated centres like Sunnybrook’s Holland Centre.
“In those particular procedures where they’ve achieved team stability, we do not see an association because the team already has a high degree of familiarity,” says Hallet.
The findings show that unlike expensive new technologies or drugs, optimising the makeup of surgical teams to foster consistency and familiarity could be a no-cost way to improve patient outcomes.
Hallet acknowledges that there are challenges and potential drawbacks to adopting a team design-centred approach to organising and scheduling surgeries. One possible consequence could be that anaesthesiologists, most of whom are currently considered generalists, become increasingly specialised and less comfortable stepping in to cover other procedures.
In the next phase of this project, the researchers are looking at this and other factors that can support the implementation of more stable teams in the operating room.
The team is currently interviewing anaesthesiologists and surgeons to understand their perspectives about the different models of care and what concerns need to be addressed to enable adoption of this new approach. They’re also doing a cost analysis to determine how much money hospitals and health systems could save by having more familiar surgical teams and fewer post-operative complications.
“You can’t put team stability or team familiarity in a bottle or replicate its effects through protocols or processes,” says Hallet.
“The only way that you can get that effect is by putting people together more often and having them work and succeed together.”
A major shift is underway in South Africa’s aesthetics industry, as cutting-edge platelet-rich fibrin (PRF) is quickly surpassing fillers or traditional platelet-rich plasma (PRP) therapy as the anti-ageing treatment of choice, delivering results that patients describe as “four times better” than its predecessor.
“Since introducing PRF into our practice, patients overwhelmingly choose it over PRP for skin rejuvenation and anti-ageing,” notes Dr Reza Mia, aesthetics expert at Anti-Aging Art in Johannesburg. “It means injecting a more potent concentrate with four times the cells to produce the results needed than previous alternatives, and subjectively, patients report it’s indeed four times better.”
A significant evolution from the once-popular “vampire facial”, PRF uses concentrated healing cells from the patient’s own blood to address an impressive range of concerns.
“When someone needs to improve their skin condition, stimulate hair growth, treat stretch marks and scarring, heal certain injuries or wounds, or even enhance intimate well-being with our P-shots and V-shots, PRF delivers some extraordinary results. For example, with our P-shots and V-shots, we’re seeing dramatic improvements in post-menopausal and post-pregnancy concerns among women, while men are achieving some enhancements in size, function, and performance,” he explains.
Turning platelets into a living filler
Through cutting-edge techniques, Dr Mia’s team turns the patient’s blood into a natural injectable filler with a blend of active cells and filler material, creating a gel-like substance. The filler is then injected back into the face or other areas where volume is needed, offering a compelling substitute for hyaluronic acid fillers, and a more powerful alternative to synthetic products.
PRP’s shorter lifespan comes from the use of anticoagulants that prevent clotting and keep the platelets inactive until they are injected. These additives thin the solution, causing it to spread quickly in the body. As a result, the treatment has less time to work and build momentum.
Because anticoagulants can interfere with the regenerative properties of platelets, they aren’t used in PRF. Instead, PRF works with the body’s natural fibrin clotting process, creating a rich concentration of platelets, healing proteins, and repair signals that trigger tissue regeneration and collagen production – helping the skin recover and appear more youthful for longer.
“These platelets stay active for roughly three weeks, instead of the 12-hour window we see with PRP. The release is gradual and the platelets have more time to work in the body, so collagen and fibronectin production is stimulated for longer. This translates into thicker skin, steadier hair-growth cycles, and a noticeably longer glow. Our clinic further uses an advanced centrifuge protocol that can achieve more than four times the platelet count from a session with PRF, packing each vial with far greater regenerative potential.”
In practice, Anti-Aging Art uses PRF to revitalise and restore wherever the skin or hair needs a boost. It’s become a go-to for smoothing fine lines, strengthening hair follicles to fill in patchy beards and thinning crowns, and refreshing postpartum skin. “Many patients who switched from PRP to PRF report they healed faster and need fewer follow-up visits, making it a preferred option.”
The recovery time is also notably shorter. “With standard microneedling, patients remain red for two to three days. With PRF, they’re red for just a day – the platelets actually accelerate their healing.”
A non-surgical breast enhancement alternative
One of the most groundbreaking applications has been for non-surgical breast enhancement. “For patients who’ve removed their implants and now have tissue laxity, or those seeking natural enhancement without surgical implants, PRF filler is a game-changer. For breast enhancement, there really isn’t an alternative, with results lasting as long as six to 12 months.”
Because PRF is taken from the patient’s own blood and then allowed to thicken into a soft gel before injection, it acts like a natural cushion inside the breast. Once placed, the gel holds its shape for a few weeks, giving an immediate subtle lift. The platelets inside also continue to release growth signals that tell the body to lay down fresh collagen and create tiny new blood vessels, so the early fullness slowly turns into real, living tissue instead of fading away like normal swelling.
“Patients like that the injected material is completely theirs, with no risk of immune rejection, hard capsules or implant leaks, while routine mammograms remain easy for radiologists to read. Most women feel only mild bruising and heaviness for a day or two, and they’re back to normal within the week.
“There is some swelling over the first few days, so patients should plan treatments well before any special events. If you choose a top-up after a year, the new PRF simply layers onto existing tissue, giving a gentle, cumulative boost without stretching the skin unnaturally.”
Treatments start around the cost of a mid-range smartphone and vary based on the extent of the area treated. Results become visible quickly but continue to improve over time, developing over three to six months as collagen rebuilds, delivering significant value compared to multiple syringes of traditional fillers or surgical options.
However, Dr Mia cautions that PRF is powerful but not magical. “Regeneration has a biological ceiling. We can thicken skin, soften scars, and enhance breasts naturally, but PRF doesn’t replace surgical intervention for augmentation. PRF also isn’t appropriate for everyone – especially anyone with active cancer in the treatment area, since the growth factors could stimulate those cells.
“But for most patients seeking a rejuvenated, youthful appearance with that coveted ‘juicy’ glow, PRF delivers results that synthetic alternatives simply can’t match,” he concludes.
Although postoperative complications, such as infections, can pose significant health risks to children after undergoing surgical procedures, timely detection following hospital discharge can prove challenging.
A new study from Northwestern University, along with other institutions, is the first to use consumer wearables to quickly and precisely predict postoperative complications in children and shows potential for facilitating faster treatment and care. The study appears in Science Advances.
“Today, consumer wearables are ubiquitous, with many of us relying on them to count our steps, measure our sleep and more,” said senior author Arun Jayaraman, professor at Northwestern University Feinberg School of Medicine and a scientist at Shirley Ryan AbilityLab. “Our study is the first to take this widely available technology and train the algorithm using new metrics that are more sensitive in detecting complications. Our results suggest great promise for better patient outcomes and have broad implications for paediatric health monitoring across various care settings.”
How the study worked
As part of the study, commercially available Fitbit devices were given to 103 children for 21 days immediately after appendectomy, the most common surgery in children, which results in complications up to 38% of the time. Rather than just using the metrics automatically captured by the Fitbit to identify signs of complications (eg, low activity, high heart rate, etc.), Shirley Ryan AbilityLab scientists trained the algorithm using new metrics related to the circadian rhythms of a child’s activity and heart rate patterns.
In the process, they found such metrics were more sensitive to picking up complications than the traditional metrics. In fact, in analysing the data, scientists were able to retrospectively predict postoperative complications up to three days before formal diagnosis with 91% sensitivity and 74% specificity.
“Historically, we have been reliant upon subjective reporting from children – who often have greater difficulty articulating their symptoms – and their caregivers following hospital discharge. As a result, complications are not always caught right away,” said study author Dr Fizan Abdullah, who at the time of the study was an attending physician of paediatric surgery at Ann & Robert H. Lurie Children’s Hospital of Chicago and a professor at Feinberg. “By using widely available wearables, coupled with this novel algorithm, we have an opportunity to change the paradigm of postoperative monitoring and care – and improve outcomes for kids in the process.”
What’s next?
This research is part of a four-year National Institutes of Health-funded project. As a next step, scientists plan to transition this approach into a real-time (vs retrospective) system that analyses data automatically and sends alerts to children’s clinical teams.
“This study reinforces wearables’ potential to complement clinical care for better patient recoveries,” said Hassan M.K. Ghomrawi, vice chair of research and innovation in the department of orthopaedic surgery at University of Alabama at Birmingham. “Our team is eager to enter the next phase of research exploration.”
A medical team at Erasmus University Medical Center in the Netherlands uses the new imaging probe with a Quest camera to get a better view of cancerous tumors during non-brain cancer surgery. Photo courtesy of Erasmus University Medical Center
In a significant leap forward for successful cancer surgery, researchers at the University of Missouri and collaborators have developed a new imaging probe to help surgeons more accurately identify and remove aggressive tumours during operations.
The tool is expected to be a critical advancement in the fight against glioblastoma, one of the most difficult-to-treat brain cancers. In the future, it is intended to be expanded for image-guided surgery of various other solid tumours.
Described in a new study in Nature Publishing Group Imaging, the innovation works by pairing a fluorescent dye with a fatty acid molecule that cancer cells readily absorb. When introduced into the body, the compound is taken up by tumour cells, causing them to glow under near-infrared light, revealing cancer that might otherwise remain hidden.
Glioblastoma is considered surgically incurable because the tumour doesn’t stay in one place – it spreads and invades healthy brain tissue in a diffuse, microscopic way. This makes it impossible to remove completely without risking serious damage to brain function.
“Surgery remains one of the primary treatments for many cancers,” Elena Goun, associate professor of chemistry in the College of Arts and Science and one of the lead authors of the study, said. “In breast or prostate cancer, surgeons can often remove the tumour along with surrounding tissue. In brain cancer, that’s simply not possible. You must preserve healthy brain tissue. But if even a few cancer cells are left behind, the disease will return.”
That dilemma is especially acute with glioblastoma, which doesn’t form a neatly contained mass. Instead, it sends out microscopic extensions — finger-like projections that blend into healthy brain tissue and are invisible to the naked eye.
Because of this, surgeons must walk a fine line: removing as much tumour as possible while avoiding harm to vital brain areas. The more thoroughly the tumour is removed, the more effective follow-up treatments like radiation and chemotherapy tend to be.
The new small-molecule probe, known as FA-ICG, is engineered to solve that problem. It links a natural long-chain fatty acid (FA) to indocyanine green (ICG), an FDA-approved near-infrared dye widely used in surgical imaging. This fatty acid-based approach means the probe is highly selective: glioblastoma cells, which thrive on fatty acids, absorb it more than normal brain cells. That makes the cancer stand out more clearly.
The result is a tool that takes advantage of cancer’s altered metabolism to highlight tumour cells from within.
“Surgeons would view a monitor during surgery showing where the probe is lighting up,” Goun explained. “If they still see fluorescent signals, it means cancer is still present and more tissue needs to be removed. When the light disappears, they would know they’ve cleared the area.”
In the operating room, surgeons already use a variety of tools to guide tumour removal – including microscopes, ultrasound and fluorescent dyes. Of those, fluorescent dyes are particularly useful because they make otherwise invisible tumour cells light up under special lighting.
Right now, the only approved imaging dye for glioblastoma surgery is 5-ALA, which fluoresces under blue light. But 5-ALA comes with major limitations: The operating room must be darkened in order to see it, tissue penetration is shallow and the fluorescent signal is often weak and non-specific.
It also comes with side effects, including photosensitivity, meaning patients must avoid bright light exposure after surgery due to the risk of skin and eye damage.
That’s where the FA-ICG probe shines – both literally and functionally.
Compared to 5-ALA, FA-ICG is brighter, works under normal surgical lighting, and offers real-time visualisation under the microscope – no need to turn the lights off mid-surgery. This saves time and makes procedures more efficient. The signal-to-background ratio is also higher, meaning it’s easier to distinguish tumour tissue from healthy brain.
The FA-ICG probe is not only easier to see, it’s also easier to use. Its longer half-life allows more flexibility in scheduling surgeries, and the logistics of administration are simpler than with current probes.
“The upside of fluorescence-guided surgery is that you can make little remnants much more visible using the light emitting properties of these tumour cells when you give them a dye,” said Rutger Balvers, a neurosurgeon at Erasmus University Medical Center in the Netherlands, who is expected to lead human clinical trials of the probe. “And we think that the upside of FA-ICG compared to what we have now is that it’s more select in targeting tumour cells. The visual properties of the probe are better than what we’ve used before.”
Michael Chicoine is a neurosurgeon at MU Health Care and chair of Mizzou’s School of Medicine’s Department of Neurosurgery. While he’s not directly involved in the research, Chicoine understands the potential benefits firsthand.
Currently, he said, MRIs are the gold standard for imaging tumours; however, they’re expensive and time-consuming, especially when required during an operation.
“This fluorescent metabolically linked tool gives you real-time imaging,” he said. “We could merge techniques, using the probe during surgery and saving the MRI for a sort of final exam. It’s definitely an exciting advancement.”
Researchers are also excited about other uses for the probe, including for other types of cancers and for use during follow-up treatments.
“After radiation or chemotherapy, it becomes very difficult to distinguish between scar tissue and active tumor,” Chicoine said. “This probe could give us a definitive answer – helping doctors know whether to continue treatment or adjust it, or consider another surgery. Eliminating the current uncertainty would be really helpful.”
Another promising use of the probe could be in photodynamic therapy either during or after surgery. Since the dye also has light-activated properties that can kill cancer cells, researchers are exploring whether it could double as a treatment tool, not just a diagnostic one.
Clinical trials for use in glioblastoma cases are expected to start in Europe, with strong interest already growing among neurosurgical teams.
The upcoming Phase 1 trial will focus on how patients tolerate the probe, whether there are any side effects at an effective dose and how its performance compares to existing tools. Ultimately, the goal is to make brain tumour surgery safer, helping surgeons remove all cancerous tissues while preserving as much healthy brain tissue as possible.
If results are positive, future studies could expand the use of FA-ICG beyond brain tumours to other cancers with high fatty acid metabolism, such as pancreatic cancer,according to fellow corresponding author Laura Mezzanotte from the Erasmus’ Department of Radiology and Nuclear Medicine.
Self-esteem scores more than doubled within one year of weight-loss surgery, according to a new study* presented at the American Society for Metabolic and Bariatric Surgery (ASMBS) 2025 Annual Scientific Meeting.
Researchers from Geisinger Medical Center found that after bariatric surgery self-esteem scores rose to 77.5 from 33.6 – a more than 40-point increase. The higher the score on a scale from 0 to 100, the higher the level of self-esteem and quality of life. The amount of weight loss appears to fuel the increase in self-esteem — scores were highest among those who lost the most weight despite demographics differences including gender, age, and race or type of bariatric procedure.
Researchers used a prospectively maintained database to identify 5,749 patients aged 18 and older with body mass index (BMI) of 35 or more who had metabolic and bariatric surgery between 2006 and 2019. Patients completed the Impact of Weight Quality of Life (iwQOL) survey pre-operatively and 12 months after the operation to assess weight stigma and their quality of life.
“Understanding weight stigma and psychosocial factors associated with obesity is essential to offering holistic care. While these factors should not dictate the decision to have bariatric surgery, they should be an important part of the conversation,” said study co-author Justin Dhyani, MD, Geisinger Medical Center in Danville, PA.
Weight stigma is associated with adverse health outcomes including depression, anxiety, disordered eating, and low self-esteem. Among adults with obesity, the prevalence of weight discrimination is 19% to 42%, with higher rates reported among those with higher BMIs and women.
“Weight stigma is a serious issue that places an extra psychological burden on patients struggling with obesity and there is no excuse for it,” said Ann M. Rogers, MD, MD, FACS, FASMBS, President, ASMBS, who was not involved in the study. “This study shows we need to understand what patients are going through and be supportive and empowering of them as they navigate their health and make decisions about treatment.”