A cortical neuron treated with JRT, a synthetic molecule similar to the psychedelic drug LSD. Drugs like JRT might enable new treatments for conditions such as schizophrenia, without the hallucinations and other side effects of psychedelics. (Photo credit: Lee E. Dunlap, Institute for Psychedelics and Neurotherapeutics, UC Davis)
University of California, Davis, researchers have developed a new, neuroplasticity-promoting drug closely related to LSD that harnesses the psychedelic’s therapeutic power with reduced hallucinogenic potential.
The research, published in PNAS, highlights the new drug’s potential as a treatment option for conditions like schizophrenia, where psychedelics are not prescribed for safety reasons. The compound also may be useful for treating other neuropsychiatric and neurodegenerative diseases characterised by synaptic loss and brain atrophy.
To design the drug, dubbed JRT, researchers flipped the position of just two atoms in LSD’s molecular structure. The chemical flip reduced JRT’s hallucinogenic potential while maintaining its neurotherapeutic properties, including its ability to spur neuronal growth and repair damaged neuronal connections that are often observed in the brains of those with neuropsychiatric and neurodegenerative diseases.
“Basically, what we did here is a tire rotation,” said corresponding author David E. Olson, director of the Institute for Psychedelics and Neurotherapeutics and a professor of chemistry, and biochemistry and molecular medicine at UC Davis. “By just transposing two atoms in LSD, we significantly improved JRT’s selectivity profile and reduced its hallucinogenic potential.”
JRT exhibited powerful neuroplastic effects and improved measures in mice relevant to the negative and cognitive symptoms of schizophrenia, without exacerbating behaviours and gene expression associated with psychosis.
“No one really wants to give a hallucinogenic molecule like LSD to a patient with schizophrenia,” said Olson, who is also co-founder and chief innovation officer of Delix Therapeutics, a company that aims to bring neuroplastogens to the market. “The development of JRT emphasises that we can use psychedelics like LSD as starting points to make better medicines. We may be able to create medications that can be used in patient populations where psychedelic use is precluded.”
Testing JRT’s potential
Olson said that it took his team nearly five years to complete the 12-step synthesis process to produce JRT. The molecule was named after Jeremy R. Tuck, a former graduate student in Olson’s laboratory, who was the first to synthesise it and is a co-first author of the study along with Lee E. Dunlap, another former graduate student in Olson’s laboratory.
Following JRT’s successful synthesis, the researchers conducted a battery of cellular and mouse assays that demonstrated the drug’s neuroplastic effects and improved safety profile relative to LSD.
Key findings included:
JRT and LSD have the exact same molecular weight and overall shape, but distinct pharmacological properties.
JRT is very potent and highly selective for binding to serotonin receptors, specifically 5-HT2A receptors, the activation of which are key to promoting cortical neuron growth.
JRT promoted neuroplasticity, or growth between cellular connections in the brain, leading to a 46% increase in dendritic spine density and an 18% increase in synapse density in the prefrontal cortex.
JRT did not produce hallucinogenic-like behaviors that are typically seen when mice are dosed with LSD.
JRT did not promote gene expression associated with schizophrenia. Such gene expression is typically amplified with LSD use.
JRT produced robust anti-depressant effects, with it being around 100-fold more potent than ketamine, the state-of-the-art fast-acting anti-depressant.
JRT promoted cognitive flexibility, successfully addressing deficits in reversal learning that are associated with schizophrenia.
“JRT has extremely high therapeutic potential. Right now, we are testing it in other disease models, improving its synthesis, and creating new analogues of JRT that might be even better,” Olson said.
A more effective treatment for schizophrenia
Olson emphasised JRT’s potential for treating the negative and cognitive symptoms of schizophrenia, as most current treatments produce limited effects on anhedonia — the inability to feel pleasure — and cognitive function. Clozapine is the one exception, but it has side effects, and is not first-line drug of choice for people with severe schizophrenia.
Olson and his team are currently testing JRT’s potential against other neurodegenerative and neuropsychiatric diseases.
Neisseria gonorrhoeae Bacteria Scanning electron micrograph of Neisseria gonorrhoeae bacteria, which causes gonorrhea. Captured by the Research Technologies Branch (RTB) at the NIAID Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID. Photo by National Institute of Allergy and Infectious Diseases on Unsplash
By Catherine Tomlinson
Two new antibiotics offer hope for people with gonorrhoea that is resistant to currently available drugs. Yet, it might be years before the people who need these medicines can get them. Spotlight unpacks why these new antibiotics are important and what needs to happen before they can be used in South Africa.
Gonorrhoea is a sexually transmitted infection known for its ability to quickly mutate to evade the antibiotics used to treat it. Its symptoms include pain when urinating and genital discharge, but many people don’t notice any symptoms at all. If gonorrhoea is not treated, it can cause serious problems including infertility, chronic pain and complications in babies who risk developing infections that can cause eye damage and blindness.
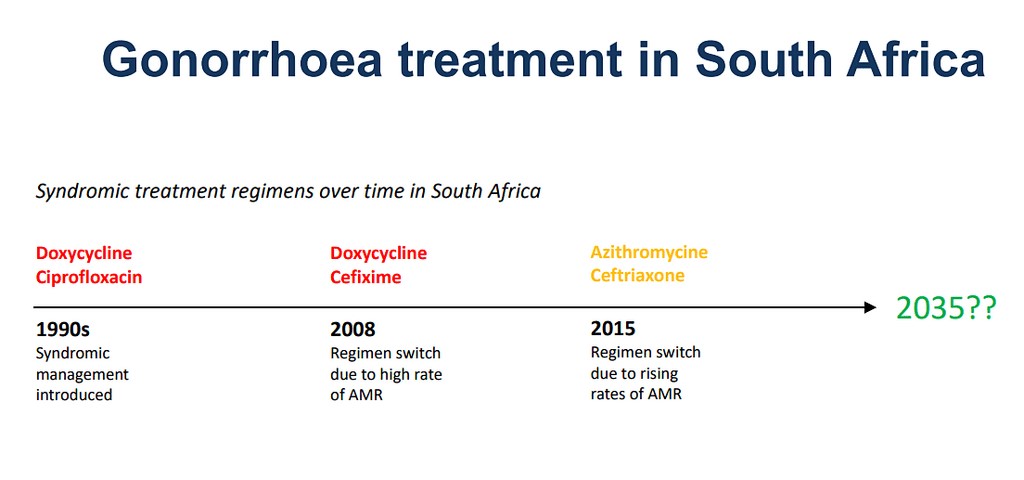
Gonorrhoea treatment has been something of a cat-and-mouse game as the bacteria continuously developed resistance against the antibiotics used to treat it. From the 1990s to the early 2000s, the antibiotic ciprofloxacin was used to treat gonorrhoea in South Africa, sometimes combined with another one called doxycycline. But as high levels of ciprofloxacin resistance emerged, South Africa replaced this course of therapy with a regimen of cefixime and doxycycline. Gonorrhoea treatment was changed again in 2015, due to concerns regarding the emergence of cefixime-resistance.
The treatment regimen adopted in 2015 remains the standard of care in South Africa and much of the world today. It involves an intermuscular injection of ceftriaxone, combined with oral azithromycin pills. Although, some countries now recommend using high dose injectable ceftriaxone on its own, due to high levels of azithromycin resistance.
While most gonorrhoea cases are still treatable with ceftriaxone, the emergence of ceftriaxone-resistant gonorrhoea has been identified as a major global health threat.
“The last effective drug we have, ceftriaxone, already indicates increasing gonococcal resistance. Without new antibiotics, we will have no easy treatment options. This is a great concern that will have a major impact in disease control efforts,” warned the World Health Organization (WHO).
This is why two new antibiotics, zoliflodacin and gepotidacin, are considered such a big deal. They are the first new medicines developed for gonorrhoea in over 30 years. Both are in new classes of antibiotics, which is to say they attack the bacterium in a different way than previous medicines. Because of this, they have little cross resistance with existing treatments and therefore offer important treatment options for people for whom the old medicines no longer work.
How widespread is ceftriaxone-resistance in South Africa?
How urgently we need access to the new medicines in South Africa will depend largely on how many people here are resistant to ceftriaxone. Unfortunately, we don’t have a clear picture of drug-resistant gonorrhoea in the country.
South Africa introduced a syndromic management approach for sexually transmitted infections (STIs) in the mid-1990s, as recommended by the WHO. This means that people reporting STI symptoms at health facilities are treated according to their symptoms, rather than results of a lab test.
This approach to STIs helps to reduce the cost burden of laboratory diagnosis and allows for immediate treatment initiation without waiting for laboratory results since some patients are “lost” over this period as they do not return to health facilities for their test results and treatment.
A challenge with treating STIs according to symptoms rather than laboratory results is that many STIs present with similar symptoms. This can lead to misdiagnosis and incorrect treatment as well as asymptomatic infections going undiagnosed and untreated.
Thus, without lab testing, combined with routine STI screening to identify asymptomatic cases, it is difficult to understand the true burden of gonorrhoea in the country or to measure the extent of drug resistance.
A systematic review, however, indicates that while azithromycin resistance is a challenge in South Africa, there was not yet evidence of ceftriaxone resistance as of 2022.
The National Institutes of Communicable Diseases (NICD) classified ceftriaxone-resistant gonorrhoea a notifiable condition in 2017, meaning that any diagnosed cases must be reported to it. The NICD did not respond to a query from Spotlight as to whether there have been any confirmed cases of ceftriaxone-resistant gonorrhoea in South Africa to date.
While South Africa is not yet facing a ceftriaxone-resistance crisis, experts are of the view that it is only a matter of time before this public health challenge reaches our borders, as global cases are increasing and the drug-resistant strain is transmittable.
Some access to zoliflodacin
Given the risk of a ceftriaxone-resistance crisis, it is important that the two new antibiotics, zoliflodacin and gepotidacin, become available here as soon as possible. These new antibiotics have quite different histories.
Zoliflodacin was developed by GARDP – a non-profit organisation working to accelerate the development of new antibiotics – together with the private biopharmaceutical company Innoviva.
In November 2023, GARDP shared the results of its phase 3 trial of zoliflodacin, which took place in South Africa, Thailand, Belgium, the Netherlands and the United States. It tested the effectiveness of a single dose of oral zoliflodacin compared with the current standard of care treatment for gonorrhoea, which is an injection of ceftriaxone combined with oral azithromycin.
The trial showed that a single dose of zoliflodacin works just as well as the standard of care. The results have not yet been published in a peer-reviewed journal.
Zoliflodacin has also “been shown to be active against all multidrug-resistant strains of Neisseria gonorrhoeae (the gonorrhoea bacteria), including those resistant to ceftriaxone, the last remaining recommended antibiotic treatment”, GARDP’s R&D Project Leader for STIs, Pierre Daram, told Spotlight.
He added that Innoviva is in the process of applying to get the greenlight to use zoliflodacin in the United States. At the same time, GARDP is planning to apply for approval in some of its own regions, starting with Thailand and South Africa.
GARDP is also working on a programme to make the unregistered drug available for patients who have no other treatment options.
“The zoliflodacin managed access programme is about to be activated,” Daram said. “The aim is to provide early access to zoliflodacin, prior to regulatory approval in a country, in response to individual patient requests by clinicians and whereby certain regulatory and clinical criteria are met.” South Africa will be one of the countries covered under this programme, said Daram.
He explained that individual patient requests for treatment will be received from treating clinicians through an online platform. “Based on information provided by the clinician and certain pre-determined regulatory and clinical criteria being met, GARDP will make a case-by-case decision as to whether zoliflodacin will be made available.” Daram added: “Consideration is given to both clinical as well as diagnostic criteria for documentation of treatment failure.”
Access to gepotidacin remains uncertain
Shortly after results for zoliflodacin were announced, GlaxoSmithKline (GSK) also shared positive findings for their new antibiotic in treating gonorrhoea. In April 2024, the company reported that a phase 3 trial showed that taking two doses of oral gepotidacin worked just as well as the standard treatment.
The results of this trial, which was conducted in Australia, Germany, Mexico, Spain, the United Kingdom, and the United States, were published in the Lancet medical journal in May.
While gepotidacin represents an important new treatment option for gonorrhoea, there is no indication that it will be available in South Africa any time soon.
Gepotidacin has not yet been registered for the treatment of gonorrhoea but was approved in March in the United States for treating uncomplicated urinary tract infections (UTIs) in women and girls over 12. The medicine will thus have a much larger market in the US than if it was only registered for treating gonorrhoea.
The price that GSK will charge for gepotidacin has not yet been disclosed, but a spokesperson told Spotlight it is set to be launched in the US in the second half of 2025.
“[T]he price in the US will be disclosed when the product will be commercialized,” said the GSK spokesperson.
The company did not respond to Spotlight’s questions regarding the company’s plans to register and market gepotidacin in South Africa.
What happens next?
With the launch of the zoliflodacin managed access programme, clinicians in South Africa will soon be able to apply for the medicine for patients that are resistant to existing drugs. Given that ceftriaxone-resistance is rare in the country, the number of patients in the country that will be eligible for zoliflodacin is likely to be small.
Securing broader access to zoliflodacin or gepotidacin, potentially for use as a first line gonorrhoea treatment appears to be a long way off. While GARDP is planning to file for registration of zoliflodacin in South Africa, GSK has not indicated whether they will follow suit for gepotidacin.
Providing the new antibiotics for first line gonorrhoea treatment could expand delivery and uptake, as the new drugs are both oral tablets and would remove the need for an injection to treat gonorrhoea, said Professor Nigel Garrett, who is the Chief Scientific Officer at the Desmond Tutu Health Foundation.
If zoliflodacin and gepotidacin are approved and made affordable in South Africa, they could also play a vital role in strengthening the country’s efforts to preserve the long-term effectiveness of other antibiotics.
Ceftriaxone “is a really important drug to keep, [to] make sure that there isn’t too much resistance against it,” Garret told Spotlight. He explained that the medicine is needed to treat sepsis occurring in hospitals, as well as meningitis.
Aortic valve narrowing (aortic stenosis) with concomitant cardiac amyloidosis is a severe heart disease of old age that is associated with a high risk of death. Until now, treatment has consisted of valve replacement, while the deposits in the heart muscle, known as amyloidosis, often remain untreated. An international research consortium led by MedUni Vienna and University College London has shown for the first time that combined treatment consisting of heart valve replacement and specific drug therapy offers a significant survival advantage for patients. The study results have been published in the European Heart Journal.
As part of the study conducted by the research team led by Christian Nitsche (MedUni Vienna) and Thomas Treibel (University College London), data from 226 patients with aortic stenosis and concomitant cardiac amyloidosis from ten countries were examined. Aortic stenosis is a narrowing of the heart valve that directs blood from the left ventricle into the bloodstream. In cardiac amyloidosis, misfolded proteins are deposited in the heart muscle. Both diseases occur in older people and often together. Until now, it was unclear whether treating amyloidosis in addition to valve surgery would benefit patients.
The analysis now published showed that both aortic valve replacement and treatment with the drug tafamidis for amyloidosis were associated with a significantly lower risk of death. The survival benefit was highest in patients who received both forms of treatment. “Our results even show that patients with both conditions who received valve replacement and specific amyloidosis therapy had similar long-term survival rates to people with aortic stenosis without amyloidosis,” emphasises study leader Christian Nitsche.
Targeted tests necessary
Both aortic stenosis and cardiac amyloidosis impair the heart’s pumping function and can lead to death if left untreated. Targeted therapy can slow the progression of amyloidosis, while valve replacement treats the mechanical stress caused by the narrowed heart valve. Around ten percent of patients with aortic stenosis also have amyloidosis, but this is often not diagnosed in everyday clinical practice. “Our findings also suggest that patients with severe aortic valve stenosis should be screened for amyloidosis so that we can offer them targeted life-prolonging treatment options,” emphasises Christian Nitsche.
Chronic inflammatory bowel disease is challenging to treat and carries a risk of complications, including the development of bowel cancer. Young people are particularly affected: when genetic predisposition and certain factors coincide, diseases such as ulcerative colitis or Crohn’s disease usually manifest between the ages of 15 and 29 – a critical period for education and early career development. Prompt diagnosis and treatment are crucial. Researchers at Charité – Universitätsmedizin Berlin have now discovered a therapeutic target that significantly contributes to halting the ongoing inflammatory processes. Their findings are published in the current issue of the journal Nature Immunology*.
Sometimes gradually, sometimes in flare-ups – accompanied by severe abdominal cramps, diarrhoea, weight loss, fatigue and a high level of emotional stress – this is how the two most common chronic inflammatory bowel diseases, Crohn’s disease and ulcerative colitis, often begin. While ulcerative colitis only affects the inner lining of the large intestine, Crohn’s disease can involve the entire thickness of the intestinal wall, most commonly in the small intestine, but sometimes also the stomach and oesophagus. Ongoing inflammation can cause lasting tissue damage and increase the risk of cancer. While traditional treatments aim to suppress the immune system as a whole, newer therapies are more targeted: they interrupt the inflammatory process by blocking specific messenger substances that drive inflammation in the body.
The exact causes of severe systemic diseases are still not fully understood. In addition to genetic factors, environmental influences are also believed to play an important role in their development. Prof Ahmed Hegazy has been studying inflammatory processes in the gut and the immune system’s defence mechanisms at Charité’s Department of Gastroenterology, Infectiology and Rheumatology for several years. Together with his team, he has now succeeded in identifying the interaction between two messenger substances of the immune system as the driving force behind chronic intestinal inflammation: Interleukin-22, a protein that supports the cells lining the inside of the gut and helps maintain the protective barrier, and oncostatin M, a signalling molecule that plays a significant role in tissue repair and cell differentiation.
Uncontrolled chain reaction
“At the clinic, we mainly see young patients who just beginning their professional lives. So far, we have only been able to slow down the progression of the disease and alleviate symptoms. But not all patients respond well to existing treatments, so new therapeutic approaches are urgently needed,” says Ahmed Hegazy. In previous work, the research team closely examined the effects of oncostatin M, an inflammation-promoting messenger molecule. This protein, produced by certain immune cells, activates other inflammatory factors – setting off a chain reaction that triggers an excessive immune response. “It was especially interesting for us to see that patients with high levels of oncostatin M do not respond to several common therapies,” Ahmed Hegazy explains. “This means that Oncostatin M levels could help predict treatment failure and may serve as a biomarker for more severe disease. That’s exactly where we focused our efforts: we wanted to understand this signaling pathway better and find ways to block it with targeted treatments.”
The research team spent five years uncovering how the immune messenger oncostatin M triggers inflammatory responses. They began by using animal models, and later studies tissue samples from patients, to examine the different stages of chronic intestinal diseases, State-of-the-art single-cell sequencing showed that – compared to healthy tissue – a much larger number of unexpected cell types in the inflamed gut have receptors for oncostatin M. At the same time, additional immune cells start producing the inflammatory protein. Interestingly, interleukin-22, which normally protects tissue, also makes the gut lining more sensitive to oncostatin M by increasing the number of its receptors. “These two immune messengers work together and amplify the inflammation, drawing more immune cells into the intestine, like a fire that keeps getting more fuel and spreads,” as Ahmed Hegazy relates. “In our models, we specifically blocked the binding sites for oncostatin M and saw a clear reduction in both chronic inflammation and the associated of cancer.”
Targeted therapy for high-risk patients in sight
The researchers found a particularly high number of receptors for the messenger molecule oncostatin M around the tumours in tissue samples from patients with colorectal cancer caused by chronic intestinal inflammation, but not in the surrounding healthy tissue. This observation suggests that this signalling pathway may help promote cancer development. But chronic inflammation does not always lead to bowel cancer, and not every patient is affected in the same way, making treatment and prognosis difficult. With an understanding of oncostatin M’s amplifying effect on interleukin-22, new therapies may be possible.
The team’s experimental findings may soon translate into a real-world therapy: by specifically disrupting the harmful interaction between the immune messengers interleukin-22 and oncostatin M. “Our results provide a strong scientific basis for developing targeted treatments against this inflammation-promoting mechanism in chronic inflammatory bowel disease — particularly in patients with more severe forms of the illness,” explains Ahmed Hegazy. A clinical trial is already underway to test an antibody that blocks the receptors for Oncostatin M.
Elated at graduating with a doctoral degree is Dr Aviwe Ntsethe. Credit: University of KwaZulu-Natal
Dr Aviwe Ntsethe’s curiosity in the Medical field deepened when he started exploring the complexities of human physiology and the crucial role of the immune system in cancer, leading to him graduating with a PhD.
Growing up in the small town of Bizana in the Eastern Cape, Ntsethe attended Ntabezulu High School, where his passion for Medical Science took root. Despite facing significant challenges, including limited funding opportunities for his studies, he remained determined to advance in the discipline.
Throughout his PhD journey at UKZN, Ntsethe had to juggle multiple jobs to support himself and his studies while conducting his research. He worked at Netcare Education and the KwaZulu-Natal College of Emergency Care, and later took up a position as a contractual laboratory technician in the Department of Physiology at UKZN. It was with the guidance of his PhD supervisor, Professor Bongani Nkambule, that he learned critical work ethics and advanced laboratory techniques. The co-supervision of Professor Phiwayinkosi Dludla further enriched his research experience and contributed to his academic growth.
Ntsethe’s thesis focused on investigating B cell function and immune checkpoint expression in patients with Chronic Lymphocytic Leukaemia (CLL). The study found that patients with CLL had higher levels of immune checkpoint proteins in their B cell subsets, which play a crucial role in regulating the immune system.
Furthermore, using monoclonal antibodies that target these immune checkpoints, he found these patients could potentially benefit from immunotherapy. Specifically, immunotherapy may improve the function of B cells, key players in fighting infections and cancers, thereby offering new hope for better outcomes in patients with CLL.
He has published three papers from this study. ‘I am excited and proud when I reflect on my achievement of completing this significant journey which was both challenging and rewarding, pushing me to expand my knowledge and skills in ways I never imagined.’
Now, a lecturer at Nelson Mandela University, Ntsethe is committed to mentoring the next generation of Medical scientists. He continues to use the invaluable knowledge and experience he gained during his PhD studies to inspire students and cultivate their passions in research and health sciences. Looking ahead, Ntsethe hopes to expand his research, focusing on immune system interactions in chronic diseases while also encouraging students from diverse backgrounds to pursue careers in Medical Science.
Outside academia, Ntsethe enjoys travelling, staying physically active through workouts, playing chess and indulging in coding or programming.