A study in stroke patients shows the brain’s vision-language connection shapes object knowledge
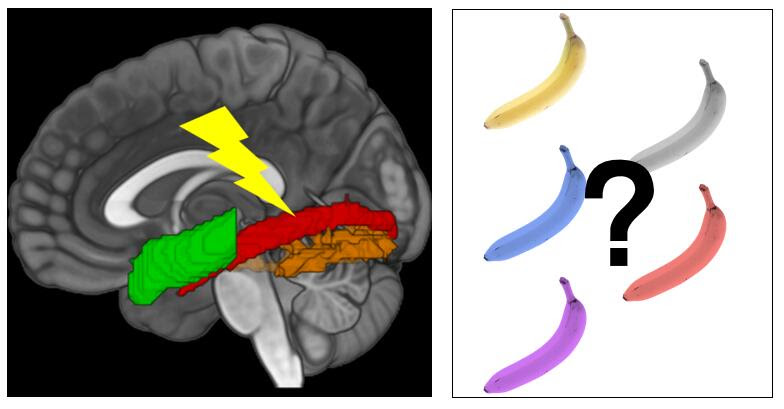
A schematic view of the main findings, adapted from a brain figure in the study. Image credit: Adapted from Liu Bet al., 2025, PLOS Biology, CC-BY 4.0
Our ability to store information about familiar objects depends on the connection between visual and language processing regions in the brain, according to a study published May 20th in the open-access journal PLOS Biology by Bo Liu from Beijing Normal University, China, and colleagues.
Seeing an object and knowing visual information about it, like its usual colour, activate the same parts of the brain. Seeing a yellow banana, for example, and knowing that the object represented by the word “banana” is usually yellow, both excite the ventral occipitotemporal cortex (VOTC). However, there’s evidence that parts of the brain involved in language, like the dorsal anterior temporal lobe (ATL), are also involved in this process – dementia patients with ATL damage, for example, struggle with object colour knowledge, despite having relatively normal visual processing areas. To understand whether communication between the brain’s language and sensory association systems is necessary for representing information about objects, the authors tested whether stroke-induced damage to the neural pathways connecting these two systems impacted patients’ ability to match objects to their typical colour. They compared colour-identification behaviour in 33 stroke patients to 35 demographically-matched controls, using fMRI to record brain activity and diffusion imaging to map the white matter connections between language regions and the VOTC.
The researchers found that stronger connections between language and visual processing regions correlated with stronger object color representations in the VOTC, and supported better performance on object color knowledge tasks. These effects couldn’t be explained by variations in patients’ stroke lesions, related cognitive processes (like simply recognizing a patch of color), or problems with earlier stages of visual processing. The authors suggest that these results highlight the sophisticated connection between vision and language in the human brain.
The authors add, “Our findings reveal that the brain’s ability to store and retrieve object perceptual knowledge – like the colour of a banana – relies on critical connections between visual and language systems. Damage to these connections disrupts both brain activity and behaviour, showing that language isn’t just for communication – it fundamentally shapes how sensory experiences are neurally structured into knowledge.”
As the world marks Nurses Day this month, this annual anniversary has shone a sharp spotlight on the realities facing this group of South African heroes and heroines. With many battling burnout, bracing for further staff shortages and trying to find ways to absorb the impact of global funding cuts, Fundi is inviting the country to get behind our nurses and celebrate their daily untold contribution to our local communities.
Recent announcements by the United States to slash foreign aid to global health programmes (including PEPFAR, which funds major HIV initiatives in South Africa) sent shockwaves through our local healthcare sector.
“For nurses already stretched to breaking point, this was yet another blow,” notes Mary Maponya, Fundi Executive Head: Lending. “This isn’t just about money disappearing from a spreadsheet. It’s about support being taken from clinics, treatment delays growing longer and nurses being asked to pick up even more of the slack. We need to acknowledge that nurses are the pulse of public healthcare in South Africa – and that pulse is under pressure.”
Maponya says this is why it was so important for Fundi to find ways to add its voice of thanks and appreciation for nurses this month – including sponsoring and attending Denosa events in Limpopo, Mpumalanga and KwaZulu-Natal. “Department of Health employees make up 16% of our total loan book, with a high proportion of these being nurses,” she explains. “They are a growing sector; continuously investing in their own self-development as a means of deepening their vocations and contribution.”
Fundi’s presence at these events made it possible to engage meaningfully with nurses on the ground; building relationships and understanding how best to continue to provide support around career advancement in particular.
“We are also be running a social media campaign until 23 May where frontline nurses can win free lunch for the week – with Uber Eats delivering it straight to their workplace to lighten the load. Small acts of kindness and appreciation make all the difference,” says Maponya. “And that’s exactly what we’re hoping this campaign will do!”
According to the South African Nursing Council, South Africa has just over 280 000 registered nurses[1], with many nearing retirement age. Meanwhile, nurse emigration is accelerating as we struggle to keep our local nurses employed and supported[2]. “It is estimated that our country will need over 100 000 new nurses by 2030 to maintain even basic healthcare coverage[3],” Maponya explains. “With the bulk of patient care still falling on nurses – from vaccinations and chronic disease management to trauma response – the pressure on these individuals is relentless.”
Amid these systemic failings, one thing is clear however: South Africa’s nurses continue showing up with grace and courage. “This was perhaps the most important take-out from the DENOSA engagement. Our nurses show-up each day – safeguarding the life and health of their patients. These remarkable individuals remain our first line of defence during pandemics, pregnancies, mental health emergencies and more. If we want a healthier South Africa, we must protect the protectors. We need to continue investing in our nurses not just during Nurses Month, but every single day,” she concludes.
People who sit or remain sedentary for more than 14 hours a day, on average, may have a higher risk of a cardiovascular event or death in the year after treatment at a hospital for symptoms of a heart attack such as chest pain, according to new research published today in the American Heart Association’s peer-reviewed scientific journal Circulation: Cardiovascular Quality and Outcomes.
Previous research from the study authors found that people who had experienced a heart attack were spending up to 12 to 13 hours each day being sedentary, defined as any awake activity that involved little-to-no physical movement. In this study, the researchers used a wrist accelerometer to track the amount of time each participant spent moving or being sedentary for a median of 30 days after discharge from a hospital’s emergency department.
Wrist accelerometers measure the acceleration of motion in three directions: forwards and backwards, side-to-side, and up and down. These measurements allowed the researchers to infer the intensity of a participant’s physical activity, and they provide more accurate measurements of the participants’ time spent moving, rather than asking participants to remember. Some examples of moderate intensity physical activities are brisk walking, water aerobics, dancing, playing doubles tennis or gardening, and examples of vigorous-intensity activities are running, lap swimming, heavy yardwork such as continuous digging or hoeing, playing singles tennis or jumping rope.
”Current treatment guidelines after a cardiac event focus mainly on encouraging patients to exercise regularly,” said study lead author Keith Diaz, Ph.D., the Florence Irving Associate Professor of Behavioral Medicine at Columbia University Medical Center in New York City, a certified exercise physiologist and a volunteer member of the American Heart Association’s Physical Activity Science Committee. “In our study, we explored whether sedentary time itself may contribute to cardiovascular risk.”
Researchers followed more than 600 adults, ages 21 to 96, treated for a heart attack or chest pain in the emergency department at a single hospital system in New York City. Participants wore a wrist accelerometer for a median of 30 consecutive days after hospital discharge to measure the amount of time they spent sitting or being inactive each day. Additional cardiac events and deaths were evaluated one year after hospital discharge via phone surveys with patients, electronic health records and the Social Security Death Index. The study was focused on understanding the risk of sedentary behavior and identifying modifiable risk factors that may improve long-term outcomes in this high-risk group.
The analysis found:
Compared to participants in the group with the highest physical activity level, those in the group with the lowest activity level had a 2.58 times higher risk of having another heart problem or dying within the next year.
Replacing 30 minutes of sedentary time with 30 minutes of moderate to vigorous physical activity, daily, reduced the risk of adverse cardiovascular events or death by 61%; replacing the sedentary time with light-intensity physical activity reduced risk by 50%; and replacing the sedentary time with 30 minutes of sleep lowered risk by 14%.
According to accelerometer data, participants in the most physically active group had average daily physical activity measures of 143.8 minutes of light physical activity; 25 minutes of moderate-to-vigorous physical activity; 11.7 hours spent sedentary; and 8.4 hours of sleep.
Participants in the least physically active group had daily averages of 82.2 minutes each day of light physical activity; 2.7 minutes of moderate-to-vigorous physical activity; 15.6 hours spent sedentary; and 6.6 hours of sleep.
Participants in the group between most and least physically active had daily averages of 109.2 minutes of light intensity physical activity; 11.4 minutes of moderate-to-vigorous intensity physical activity; 13.5 hours spent sedentary and 7.8 hours of sleep.
“We were surprised that replacing sedentary time with sleep also lowered risk. Sleep is a restorative behavior that helps the body and mind recover, which is especially important after a serious health event like a heart attack,” Diaz said. “Our study indicates that one doesn’t have to start running marathons after a cardiovascular event to see benefits. Sitting less and moving or sleeping a little more can make a real difference. More physical activity and more sleep are healthier than sitting, so we hope these findings support health professionals to move toward a more holistic, flexible and individualized approach for physical activity in patients after a heart attack or chest pain.”
Physical activity and sleep are both key components of the American Heart Association’s Life’s Essential 8, a list of health behaviours and factors that support optimal cardiovascular health. Poor sleep is a known risk factor for cardiovascular disease, which claims more lives each year in the U.S. than all forms of cancer and chronic lower respiratory disease combined, according to the American Heart Association’s 2025 Statistical Update. In addition to sleep duration, a recent scientific statement from the Association highlighted the importance of sleep continuity, sleep timing, sleep satisfaction, sleep regularity, sleep-related daytime functioning and sleep architecture in cardiometabolic health.
The study had several limitations, including that the definition of sedentary behaviour was based only on the intensity level of physical movement, meaning that the study may have overestimated the time participants spent in sedentary behaviour. Additionally, there was no information about participants’ income and characteristics of the neighbourhoods where they live, which limits the study’s ability to account for social and environmental factors, including participants’ risk of one-year cardiac events and deaths. Also, hospital discharge information about whether patients were sent home, referred to rehabilitation or referred to other care centres such as skilled nursing facilities were not collected. This limited the study’s ability to fully assess whether the patients’ settings had an impact on their recovery.
Neisseria gonorrhoeae Bacteria Scanning electron micrograph of Neisseria gonorrhoeae bacteria, which causes gonorrhoea. Captured by the Research Technologies Branch (RTB) at the NIAID Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID. Photo by National Institute of Allergy and Infectious Diseases on Unsplash
In the midst of a record high in gonorrhoea cases, the NHS is to offer a gonorrhoea vaccine to gay and bisexual men with a history of multiple partners or a sexually transmitted infection (STI), the BBC reports. The gonorrhoea vaccination, which is actually a repurposed meningococcal vaccine, is estimated only to be 30–40% effective. Research shows, however, that this will be sufficient to reduce cases and their attendant costs to the NHS.
Gonorrhoea is caused by the bacterium Neisseria gonorrhoeae and is typically transmitted by having intercourse without a condom. It can cause pain, unusual discharge, genital inflammation and infertility. Evidence has shown that the MeNZB and four-component serogroup B meningococcal (4CMenB) vaccines, designed against Neisseria meningitidis, can also offer protection against gonorrhoea.
In 2023, there were more than 85 000 cases – the highest since records began in 1918. A study published in The Lancet estimates that gonorrhoea vaccination would prevent 100 000 cases, saving the NHS £7.9 million over the next decade.
While gonorrhoea is treatable with antibiotics, resistance is growing and there is concern that it may eventually become untreatable. According to The Guardian, some cases are now “extensively drug resistant” (XDR) – not responsive to ceftriaxone or the second line of treatment. There were 17 cases of ceftriaxone-resistant gonorrhoea between January 2024 and March 2025, the UK Health Security Agency (UKHSA) reported.
Over the same period, nine XDR cases were reported, while between 2022 and 2023, there were only five.
The people most affected by gonorrhoea in the UK are the 16 to 25 age group, gay and bisexual men, and those of black and Caribbean ancestry. The study’s scenario for vaccinating at-risk populations included those who had more than five sexual partners per year or who had a positive gonorrhoea test.
The vaccine, costing about £8 per dose, is cost-effective when administered to this at-risk group of men, rather than adolescents. Despite this, clinicians will be able to offer the vaccine to anyone who, in their judgment, would benefit from it. Other vaccines such as for mpox – another STI with high transmission between gay and bisexual men – and hepatitis will also be offered.
A new study led by researchers at Tulane University suggests that people with hypertension can significantly reduce, and possibly eliminate, their increased risk of premature death by controlling several key health risk factors at once.
The study, appearing in Precision Clinical Medicine, tracked more than 70 000 people with hypertension and over 224 000 without it, using data from the UK Biobank. Researchers followed participants for nearly 14 years to understand how managing these risk factors affected early mortality, defined as dying before age 80.
The eight health risk factors evaluated in the study include: blood pressure, body mass index, waist circumference, LDL “bad” cholesterol, blood sugar, kidney function, smoking status and physical activity. Notably, researchers found that hypertensive patients who had addressed at least four of these risk factors had no greater risk of an early death than those without hypertension.
“Our study shows that controlling blood pressure is not the only way to treat hypertensive patients, because high blood pressure can affect these other factors,” said corresponding author Dr Lu Qi, professor of epidemiology at Tulane University. “By addressing the individual risk factors, we can help prevent early death for those with hypertension.”
Hypertension, defined as a blood pressure of 130mmHg or higher, is the leading preventable risk factor for premature death worldwide.
The study found that addressing each additional risk factor was associated with a 13% lower risk of early death, 12% lower risk of early death due to cancer and 21% lower risk of death due to cardiovascular disease, the leading cause of premature death globally.
“Optimal risk control” – having 7 or more of the risk factors addressed – was linked to 40% less risk of early death, 39% less risk of early death due to cancer and 53% less risk of early death due to cardiovascular disease.
“To our knowledge, this is the first study to explore the association between controlling joint risk factors and premature mortality in patients with hypertension,” Qi said. “Importantly, we found that any hypertension-related excess risk of an early death could be entirely eliminated by addressing these risk factors.”
Only 7% of hypertensive participants in the study had seven or more risk factors under control, highlighting a major opportunity for prevention. Researchers say the findings underscore the importance of personalised, multifaceted care – not just prescribing medication for blood pressure, but addressing a broader range of health behaviours and conditions.