The eye of the sleeping subject was kept open with a special fixation device to record the pupil movements for several hours. (Image: Neural Control of Movement Lab / ETH Zurich)
For the first time, researchers have been able to observe how the pupils react during sleep over a period of several hours. A look under the eyelids showed them that more happens in the brain during sleep than was previously assumed.
While eyes are typically closed in sleep, there is a flurry of activity taking place beneath the eyelids: a team of researchers, led by principal investigators Caroline Lustenberger, Sarah Meissner and Nicole Wenderoth from the Neural Control of Movement Lab at ETH Zurich, have observed that the size of the pupil fluctuates constantly during sleep. As they report in Nature Communications, sometimes it increases in size, sometimes it decreases; sometimes these changes occur within seconds, other times over the course of several minutes.
“These dynamics reflect the state of arousal, or the level of brain activation in regions that are responsible for sleep-wake regulation,” says Lustenberger. “These observations contradict the previous assumption that, essentially, the level of arousal during sleep is low.”
Instead, these fluctuations in pupil size show that even during sleep, the brain is constantly switching between a higher and lower level of activation. These new findings also confirm for humans what other research groups have recently discovered in studies on rodents, who also exhibit slow fluctuations in the activation level (known in the field as arousal).
New method for an old mystery
The regions of the brain which control the activation level are situated deep within the brainstem, making it previously difficult to directly measure these processes in humans during sleep. Existing methods are technically demanding and have not yet been established in this context. The ETH researchers’ study therefore relies on pupil measurements. Pupils are known to indicate the activation level when a person is awake. They can therefore be used as markers for the activity in regions situated deeper within the brain.
The ETH researchers developed a new method for examining the changes in people’s pupils while asleep: using a special adhesive technique and a transparent plaster, they were able to keep the eyes of the test subjects open for several hours.
“Our main concern was that the test subjects would be unable to sleep with their eyes open. But in a dark room, most people forget that their eyes are still open and they are able to sleep,” explains the study’s lead author, Manuel Carro Domínguez, who developed the technique.
Analysis of the data showed that pupil dynamics is related not just to the different stages of sleep, but also to specific patterns of brain activity, such as sleep spindles and pronounced deep sleep waves – brain waves that are important for memory consolidation and sleep stability. The researchers also discovered that the brain reacts to sounds with varying degrees of intensity, depending on the level of activation, which is reflected in the size of the pupil.
A central regulator of the activation level is a small region in the brainstem, known as the locus coeruleus. In animals, scientists have been able to show that this is important for the regulation of sleep stages and waking. The ETH researchers were unable to prove in this study whether the locus coeruleus is indeed directly responsible for pupil changes. “We are simply observing pupil changes that are related to the level of brain activation and heart activity,” Lustenberger explains.
In a follow-up study, the researchers will attempt to influence the activity of the locus coeruleus using medication, so that they can investigate how this affects pupil dynamics. They hope to discover whether this region of the brain is in fact responsible for controlling the pupils during sleep, and how changes in the level of activation affect sleep and its functions.
Using pupillary dynamics to diagnose illnesses
Understanding pupil dynamics during sleep could also provide important insights for the diagnosis and treatment of sleep disorders and other illnesses. The researchers therefore want to investigate whether pupil changes during sleep can provide indications of dysfunctions of the arousal system. These include disorders such as insomnia, post-traumatic stress disorder and possibly Alzheimer’s. “These are just hypotheses that we want to investigate in the future,” says Lustenberger.
Another goal is to make the technology usable outside of sleep laboratories, such as in hospitals where it could help to monitor waking in coma patients or to diagnose sleep disorders more accurately. The pupil as a window onto the brain could thus pave the way for new opportunities in sleep medicine and neuroscience.
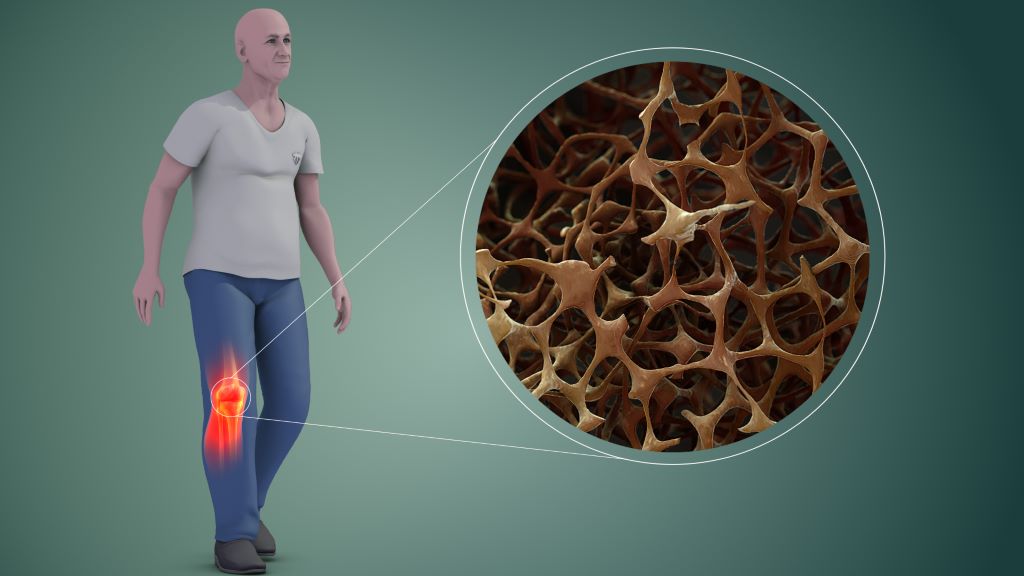
In one of the first studies of its kind, a team of researchers from Keck School of Medicine of USC has found that proteins and pathways involved in inflammation are associated with changes in bone mineral density (BMD) over time. Findings from the study were published in the Journal of Bone and Mineral Research.
The research, which was supported by the National Institutes of Health, could potentially lead to the identification of biomarkers that would serve as early indicators of a person’s risk for bone health issues later in life.
Bone mineral density is a measure of bone strength quantified by the amount of minerals in bone tissue. It peaks during young adulthood and slowly declines over the rest of the life cycle. BMD serves as an important marker for bone health and is commonly used to predict the risk of osteoporosis and other bone health conditions.
“Proteins are also substantial in the formation and maintenance of bone, and recently more studies have been trying to identify individual proteins associated with bone health,” says Emily Beglarian, the lead author and an epidemiology doctoral candidate in the Department of Population and Public Health Sciences at the Keck School of Medicine.
The study followed 304 obese/overweight Latino adolescents between the ages of 8 to 13 at baseline from the Study of Latino Adolescents at Risk for Type 2 Diabetes over an average period of three years. The researchers examined associations between over 650 proteins and annual measures of BMD, making this one of the first studies to evaluate these associations over years of follow-up. The proteins found to be associated with BMD were then inputted into a protein pathway database.
“The software determined what pathways the proteins were involved in within the human body. Our primary findings were that many of the proteins associated with BMD were involved in inflammatory and immune pathways in adolescent populations. There are other studies that found some of these same pathways were associated in older adult populations,” says Beglarian.
Existing studies suggest chronic inflammation can disrupt normal bone metabolism leading to lower BMD.
Importance of inclusive research
Childhood is a critical period for the development of BMD and this period can predict lifelong bone health.
“Until now, existing studies have centred on very specific populations. Most of them have small sample sizes, include either Chinese or non-Hispanic white populations, and focus on older adults – primarily on women because osteoporosis is four times more common in women than men,” says Beglarian.
“This is one of the first studies to investigate associations between proteins and BMD in younger populations. Investigating bone mineral density in early stages of life is important to determine how to address factors that may prevent people from reaching their potential peak bone density,” says Beglarian.
Advancing the understanding of bone health biomarkers
Additionally, Beglarian examined associations between BMD and a subset of protein markers from the initial proteins, in a separate cohort of young adults. Here she found that several proteins had similar associations with lower BMD. Low BMD is a risk factor for development of adulthood osteopenia and osteoporosis.
The study’s findings could potentially inform the development of biomarkers of bone health to identify people at risk that might benefit from intervention.
“It was interesting to see the way in which our study overlapped and differed with existing studies. Previous research was investigating BMD at the end of life when levels are already much lower,” she says. “Through my research I hope to address factors that decrease BMD earlier in life to help people get to their highest potential peak density, so they are set up over the rest of their lifetime to have a higher BMD.”
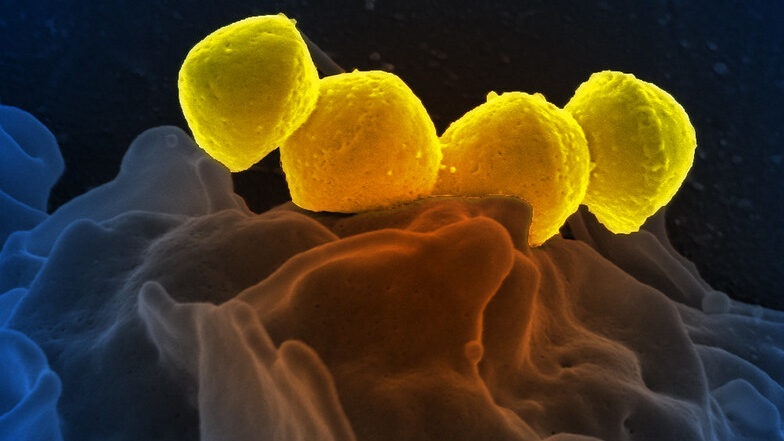
Streptococcus Pyrogenese bound To human neutrophil. Credit: NIH
A new study published in Nature Communications reveals a novel approach to mitigating tissue damage caused by Streptococcus pyogenes, the flesh-eating bacterium responsible for severe infections such as necrotising fasciitis. The research highlights how disrupting bacterial metabolism can help the body better tolerate infection and heal more effectively.
The study was led by Wei Xu, PhD, an assistant professor of biomedical sciences at the Marshall University Joan C. Edwards School of Medicine, and colleagues at Washington University School of Medicine and Central China Normal University. The team discovered that S. pyogenes manipulates the body’s immune response through its aerobic mixed-acid fermentation process, which produces metabolic byproducts, such as acetate and formate, that impair immune cell function, delay bacterial clearance and slow wound healing.
By inhibiting this bacterial metabolic pathway with a pyruvate dehydrogenase inhibitor, the team successfully reduced tissue damage in a mouse model of necrotising skin infection. These findings suggest that reprogramming bacterial metabolism could serve as a novel therapeutic approach, not only to improve host tolerance but also as a potential adjuvant therapy alongside antibiotics. This strategy could enhance the effectiveness of existing treatments, particularly in severe infections where antibiotic resistance or excessive inflammation worsens patient outcomes.
“This study sheds light on how bacterial metabolism influences the immune system,” Xu said. “By understanding these interactions, we can develop new treatment strategies that protect tissues, enhance antibiotic efficacy and improve patient outcomes.”
This effect even occurs with virtual nature – such as nature videos
Photo by Sebastian Unrau on Unsplash
In a new study, an international team of neuroscientists led by the University of Vienna has shown that experiencing nature can alleviate acute physical pain. Surprisingly, simply watching nature videos was enough to relieve pain. Using functional magnetic resonance imaging, the researchers found that acute pain was rated as less intense and unpleasant when watching nature videos – along with a reduction in brain activity associated with pain. The results, published in Nature Communications, suggest that nature-based therapies can be used as promising complementary approaches to pain management.
“Pain processing is a complex phenomenon” explains study lead and doctoral student Max Steininger from the University of Vienna. In order to better understand it and identify treatment options, Steininger and his colleagues investigated how nature exposure influences pain: participants suffering from pain were shown three types of videos: a nature scene, an indoor scene, and an urban scene. The participants rated the pain while their brain activity was measured using functional magnetic resonance imaging. The results were clear: when viewing the nature scene, the participants not only reported less pain but also showed reduced activity in brain regions associated with pain processing.
By analyzing the brain data, the researchers showed that viewing nature reduced the raw sensory signal the brain receives when in pain. “Pain is like a puzzle, made up of different pieces that are processed differently in the brain. Some pieces of the puzzle relate to our emotional response to pain, such as how unpleasant we find it. Other pieces correspond to the physical signals underlying the painful experience, such as its location in the body and its intensity. Unlike placebos, which usually change our emotional response to pain, viewing nature changed how the brain processed early, raw sensory signals of pain. Thus, the effect appears to be less influenced by participants’ expectations, and more by changes in the underlying pain signals,” explains Steininger.
Claus Lamm, head of research in the group, adds: “From another ongoing study, we know that people consistently report feeling less pain when exposed to natural environments. However, the underlying reason for this has remained unclear – until now. Our study suggests that the brain reacts less to both the physical source and the intensity of the pain.”
The current study provides important information on how nature can help alleviate pain and highlights that nature-based therapeutic approaches can be a useful addition to pain treatment. The fact, that this effect was observed by simply watching nature videos suggests that taking a walk outdoors may not be necessary. Virtual nature – such as videos or virtual reality – appears to be effective as well. This opens up a wide range of possible applications in both the private and medical sectors, providing people with a simple and accessible way to relieve their pain.
The study was conducted at the University of Vienna in collaboration with researchers from the Universities of Exeter and Birmingham (UK) and the Max Planck Institute for Human Development.
Every year, hundreds of South African children courageously battle blood disorders which are treatable through stem cell transplants. Yet, while at least 250 paediatric transplants are needed annually, only 18 are performed – leading to survival rates of just 20%, compared to 80% in countries like the USA and Europe.
Ahead of Human Rights Day, Palesa Mokomele, Head of Community Engagement and Communications at DKMS Africa, highlights the urgent need for action: “Every child has the right to healthcare, which should include stem cell transplants. By working together – government, healthcare providers, and the private sector – we can remove the barriers preventing children from receiving the treatment they need.”
Overcoming Barriers to Life-Saving Transplants
Mokomele notes that while there are challenges, there are also solutions. “By addressing issues such as financial constraints, medication shortages, and limited infrastructure, we can ensure that more children receive these vital treatments. Through collaboration, we can create meaningful change.”
Addressing the Cost Challenge
One of the major hurdles in providing this life-saving treatment is the high cost of stem cell transplants, which ranges from R1 million to R1.5 million. “When a child has a matching family donor, the public healthcare system covers their transplant fully. However, for the 70% of patients who require an unrelated donor, the state covers the transplant, but not the additional costs of finding and securing a suitable donor such as tissue typing, donor searches, and stem cell procurement.,” explains Mokomele.
“Public-private partnerships, however, can ensure that all associated costs are also covered,” she points out. “Together, we can make a difference in the lives of children who need these life-saving procedures. To be effective, we must collaborate more closely and take a holistic approach.”
Building Medical Expertise
“South Africa is challenged by the lack of clinically skilled haematology nurses and clinical haematologists, but we are looking into how ways to increase capacity at this level. Training and scholarships for medical and non-medical staff in haematology and transplantation can improve the level of care provided,” says Mokomele.
She outlines some of the work of non-profit organisations like DKMS Africa in supporting knowledge transfer initiatives for healthcare professionals. “Through a combination of theoretical courses, hands-on observerships, or a hybrid of both, we aim to enhance patient outcomes. We also frequently host and participate in symposia for the medical community to exchange knowledge and explore best practices, which are essential for providing the highest quality care.”
Encouraging Donor Commitment
A strong donor registry is crucial, yet despite DKMS Africa recruiting over 100 000 potential donors, 56% of those matched decline to donate when called upon. “Becoming a donor is a powerful act – it’s a chance to give a child a second chance at life,” urges Mokomele.”
Expanding Transplant Capacity
Increasing the number of transplant beds is another crucial step. Currently, only four paediatric transplant beds are available in public transplant centres – two in the Western Cape and two in Pretoria. However, she shares encouraging news: “We are in conversations with the private sector to support the expansion of more beds in Gauteng, where the bulk of patients reside. This expansion represents a crucial step toward improving access to care.”
A Call to Action: How You Can Help
“The progress we’re seeing is promising. Together, we can ensure that no child is denied a life-saving transplant due to financial, medical, or infrastructure constraints,” concludes Mokomele. “Whether by registering as a donor, supporting fundraising efforts, or advocating for policy changes, every contribution makes a difference. With collective effort and commitment, South Africa could transform paediatric stem cell treatment – offering hope, healing, and a future to the children who need it most.”
University of Liverpool researchers have worked with global partners to identify and successfully implement an intervention package that has significantly improved the diagnosis and management of brain infections in hospitals across Brazil, India, and Malawi.
The study, published in The Lancet, was coordinated by researchers at the University of Liverpool in collaboration with international partners and implemented across 13 hospitals.
The intervention included:
• A clinical algorithm which offered a flowchart of guidance for clinicians on how to manage the first crucial hours and days of suspected brain infections, including which tests (blood tests, lumbar puncture, brain scans) and treatments to administer. • A lumbar puncture pack, providing clinicians with sample containers, equipment, and guidance to ensure proper cerebrospinal fluid collection and testing, addressing challenges like knowing how much fluid to take and which tests to request. • A panel of laboratory tests to enable correct and timely testing for a wide range of pathogens, addressing gaps in availability and sequencing of tests, with the main goal of identifying the cause of infection. • Training for clinicians and lab staff to enhance their knowledge and skills in diagnosing and managing brain infections, including proper use of the new intervention tools.
These measures led to significant improvements in diagnosing patients with suspected acute brain infections, such as encephalitis and meningitis. Both conditions cause significant mortality and morbidity, especially in low- and middle-income countries (LMICs), where diagnosis and management are hindered by delayed lumbar punctures, limited testing, and resource constraints. Improved diagnosis and optimal management are a focus for the World Health Organization (WHO) in tackling meningitis and reducing the burden of encephalitis.
As a result of the intervention package, the proportion of patients receiving a syndromic diagnosis (confirming they had a brain infection) increased from 77% to 86%, while the microbiological diagnosis rate (identifying the exact pathogen) rose from 22% to 30%. In addition to improving diagnosis, the intervention enhanced the performance of lumbar punctures, optimised initial treatment, and improved patients’ functional recovery after illness.
Lead author Dr Bhagteshwar Singh, Clinical Research Fellow, Clinical Infection, Microbiology & Immunology said: “Following patients and their cerebrospinal fluid (CSF) samples through the hospital system, we tailored our intervention to address key gaps in care. The results speak for themselves: better diagnosis, better management, and ultimately, better outcomes for patients. Unlike most studies, we embedded improvements into routine care, so the impact continues well beyond the study.”
Corresponding author Professor Tom Solomon, Chair of Neurological Science at the University of Liverpool and Director of The Pandemic Institute, added: “We increased microbiological diagnoses by one-third across very diverse countries, which has profound implications for treatment and public health globally. As we scale this up in more hospitals and feed it into national and international policy, including WHO’s work on defeating meningitis and controlling encephalitis, the potential impact is enormous.”
The intervention was co-designed by clinicians, lab specialists, hospital administrators, researchers, and policymakers in each country, ensuring it was feasible and sustainable. Professor Priscilla Rupali, lead researcher from Christian Medical College, Vellore, India, also commented: “The co-design process ensured that the intervention would work within local healthcare settings and could be sustained beyond the study. We are already incorporating the findings into India’s national Brain Infection Guidelines, ensuring long-term benefits for patient care.”
After the US slashed global aid, the South African government stated that only 17% of its HIV spending relied on US funding. But some experts argue that US health initiatives had more bang for buck than the government’s programmes. Jesse Copelyn looks past the 17% figure, and considers how the health system is being affected by the loss of US money.
In the wake of US funding cuts for global aid, numerous donor-funded health facilities in South Africa have shut down and government clinics have lost thousands of staff members paid for by US-funded organisations. This includes nurses, social workers, clinical associates and HIV counsellors.
Spotlight and GroundUp have obtained documents from a presentation by the National Health Department during a private meeting with PEPFAR in September. The documents show that in 2024, the US funded nearly half of all HIV counsellors working in South Africa’s public primary healthcare system. The data excludes the Northern Cape.
Counsellors test people for HIV and provide information and support to those who test positive. They also follow up with patients who have stopped taking their antiretrovirals (ARVs), so that they can get them back on treatment.
Overall, the US funded 1,931 counselors across the country, the documents show. Now that many of them have been laid off, researchers say the country will test fewer people, meaning that we’ll miss new HIV infections. It also means we’ll see more treatment interruptions, and thus more deaths.
PEPFAR also funded nearly half of all data capturers, according to the documents. This amounted to 2,669 people. Data capturers play an essential role managing and recording patient files. With many of these staff retrenched, researchers say our ability to monitor the national HIV response has been compromised.
These staff members had all been funded by the US President’s Emergency Plan for AIDS Relief (PEPFAR). The funds were distributed to large South African non-government organisations (NGOs), who then hired and deployed the staff in government clinics where there is a high HIV burden. Some NGOs received PEPFAR funds to operate independent health facilities that served high-risk populations, like sex workers and LGBTQ people.
But in late January, the US paused almost all international aid funding pending a review. PEPFAR funds administered by the US Centres for Disease Control (CDC) have since resumed, but those managed by the US Agency for International Development (USAID) have largely been terminated. As a result, many of these staff have lost their jobs.
The national health department has tried to reassure the public that the country’s HIV response is mostly funded by the government, with 17% funded by PEPFAR – currently about R7.5 billion a year. But this statistic glosses over several details and obscures the full impact of the USAID cuts.
Issue 1: Some districts were heavily dependent on US funds
The first issue is that US support isn’t evenly distributed across the country. Instead, PEPFAR funding is targeted at 27 ‘high-burden districts’ – in these areas, the programme almost certainly accounted for much more than 17% of HIV spending. Some of these districts get their PEPFAR funds from the CDC, and have been less affected, but others got them exclusively from USAID. In these areas, the HIV response was heavily dependent on USAID-funded staff, all of whom disappeared overnight.
Johannesburg is one such district. A doctor at a large public hospital in this city told Spotlight and GroundUp that USAID covered a substantial proportion of the doctors, counsellors, clerks, and other administrative personnel in the hospital’s HIV clinic. “All have either had their contracts terminated or are in the process of doing so.”
The hospital’s HIV clinic lost eight counselors, eight data capturers, a clinical manager, and a medical officer (a non-specialised doctor). He said that this represented half of the clinic’s doctors and counselors, and about 80% of the data capturers.
This had been particularly devastating because it was so abrupt, he said. An instruction by the US government in late-January required all grantees to stop their work immediately.
“There was no warning about this, had we had time, we could have made contingency plans and things wouldn’t be so bad,” he explained. “But if it happens literally overnight, it’s extremely unfair on the patients and remaining staff. The loss of capacity is significant.”
He said that nurses have started to take on some of the tasks that were previously performed by counselors, such as HIV testing. But these services haven’t recovered fully and things were still “chaotic”.
He added, “It’s not as if the department has any excess capacity, so [when] nurses are diverted to do the testing and counselling, then other parts of care suffer.”
Issue 2: PEPFAR programmes got bang for buck
Secondly, while PEPFAR may only have contributed 17% of the country’s total HIV spend, some researchers believe that it achieved more per dollar than many of the health department’s programmes.
Professor Francois Venter, who runs the Ezintsha research centre at WITS university, argued that PEPFAR programmes were comparatively efficient because they were run by NGOs that needed to compete for US funding.
“PEPFAR is a monster to work for,” said Venter, who has previously worked for PEPFAR-funded groups. “They put targets in front of these organisations and say: ‘if you don’t meet them in the next month, we’ll just give the money to your competitors’ and you’ll be out on the streets … So there’s no messing around.”
US funding agencies, he said, would closely monitor progress to see if organisations were meeting these targets.
“You don’t see that with the rest of the health system, which just bumbles along with no real metrics,” said Venter.
“The health system in South Africa, like most health systems, is not terribly well monitored or well directed. When you look at what you get with every single health dollar spent on the PEPFAR program, it’s incredibly good value for money,” he said.
Not only were the programmes arguably well managed, but PEPFAR funds were also strategically targeted. Public health specialist Lynne Wilkinson provided the example of the differentiated service delivery programme. This is run by the health department, but supported by PEPFAR in one key way.
Wilkinson explained that once patients are clinically stable and virally suppressed they don’t need to pick up their ARVs from a health facility each month as it’s too time-consuming both for them and the facility. As a result, the health department created a system of “differentiated service delivery”, in which patients instead pick up their medication from external sites (like pharmacies) without going through a clinical evaluation each time. But Wilkinson noted that before someone can be enrolled in that service delivery model, clinicians need to check that patients are eligible.
“Because [the enrollment process] was going very slowly … this was supplemented by PEPFAR-funded clinicians who would go into a clinic and review a lot of clients, and get them into that system”. By doing this, PEPFAR-funded staff successfully resolved a major bottleneck in the system, she said, reducing the number of people in clinics, and thus cutting down on waiting times.
Not everyone is as confident about the overall PEPFAR model. The former deputy director of the national health department, Dr Yogan Pillay, told Spotlight and GroundUp that we don’t have data on how efficient PEPFAR programmes are at the national level. This needs to be investigated before the health department spends its limited resources on trying to revive or replicate the programmes, argued Pillay who is now the director for HIV and TB delivery at the Gates Foundation.
While he said that many PEPFAR-funded initiatives were providing crucial services, Pillay also argued that “the management structure of the [recipient] NGOs is too top-heavy and too expensive” for the government to fund. Ultimately, we need to consider and evaluate a variety of HIV delivery models instead of rushing to replicate the PEPFAR ones, he said.
Issue 3: PEPFAR supported groups that the government doesn’t reach
An additional issue obscured by the 17% figure is that PEPFAR specifically targeted groups of people that are most likely to contract and transmit HIV, like people who inject drugs, sex workers, and the LGBTQ community. These groups, called key populations, require specialised services that the government struggles to provide.
Historically, PEPFAR has given NGOs money so that they could help key populations from drop-in centres and mobile clinics, or via outreach services. All of this operated outside of government clinics, because key populations often face stigma in these settings and are thus unwilling to go there.
For instance, while about 90% of surveyed sex workers say that staff at key populations centres are always friendly and professional, only a quarter feel the same way about staff at government clinics. This is according to a 2024 report, which also found that many key populations are mistreated and discriminated against at public health facilities. (Ironically, health system monitoring organisation Ritshidze, which conducted the survey, has been gutted by US funding cuts.)
While the key populations centres funded by the CDC are still operational, those funded by USAID have closed. The health department has urged patients that were relying on these services to go to government health facilities, but researchers argue that many simply won’t do this.
Venter explained: “For years, I ran the sex worker program [at WITS RHI, which was funded by PEPFAR] … Because sex workers don’t come to [health facilities], you had to provide outreach services at the brothels. This meant … we had to deal with violence issues, we had to deal with the brothel owners, and work out which days of the week, and hours of the day we could provide the care. Logistically, it’s much more complex than sitting on your bum and waiting for them to come and visit you at the clinic.
“So you can put up your hand and say: ‘Oh they can just come to the clinics’ – like the minister said. Well, then you won’t be treating any sex workers.” Venter said this would result in a public health disaster.
He argued that one of the most crucial services that key populations may lose access to is pre-exposure prophylaxis (PrEP), a daily pill that prevents HIV.
While the vast majority of government clinics have PrEP on hand, they often fail to inform people about it. For instance, a survey of people who are at high-risk of contracting HIV in KwaZulu-Natal found that only 15% were even aware that their clinic stocked PrEP.
Another large survey found that at government facilities, only 19% of sex workers had been offered PrEP. By contrast, at the drop-in centres for key populations, the figure was more than double this, at 40%. Without these centres, the health system may lose its ability to create demand for the drug among the most high-risk groups.
One health department official told Spotlight and GroundUp that the bulk of the PrEP rollout would continue despite the US funding cuts. “The majority of the PrEP is offered through the [government] clinics,” she said, 96% of which have the drug.
However, she conceded that specific high-risk groups like sex workers have primarily gotten PrEP from the key populations centres, rather than the clinics. “This is the biggest area where we are going to see a major decline in uptake for [PrEP] services,” she said.
600 000 dead without PEPFAR?
Overall, the USAID funding cuts have severely hindered the HIV testing programmes, data capturing services, PrEP roll-out, and follow-up services for people who interrupt ARV treatment. And the patients who are most affected by this are those that are most likely to further transmit the virus.
So what will the impacts be? According to one modelling study, recently published in the Annals of Medicine, the complete loss of all PEPFAR funds could lead to over 600 000 deaths in South Africa over the next decade.
While South Africa still retains some PEPFAR funding that comes from the CDC, beneficiaries are bracing for this to end. According to Wilkinson, the PEPFAR grants of most CDC-funded organisations end in September and future grants are uncertain. For some organisations, the money stops at the end of this month.
Meanwhile, if the government has any clear plan for how to manage the crisis, it’s certainly not making this public.
In response to our questions about whether the health department would be supporting key populations centres, the department’s spokesperson, Foster Mohale, said: “For now we urge all people living with HIV/AIDS and TB to continue with treatment at public health facilities.”
When pressed for details about the department’s plans for dealing with the US cuts, Mohale simply said that they could not reveal specifics at this stage and that “this is a work in progress”.
In his budget speech in Parliament on Wednesday, Finance Minister Enoch Godongwana did not announce any funding to cover the gap left by the abrupt end of US support for the country’s HIV response. Prior to the speech, Godongwana told reporters in a briefing that the Department of Health would assist with some of the shortfall, but no further information could be provided.
Henry Adams, Country Manager South Africa, InterSystems
Healthcare data is one of the most complex and valuable assets in the modern world. Yet, despite the wealth of digital health information being generated daily, many organisations still struggle to access, integrate, and use it effectively. The promise of data-driven healthcare – where patient records, research insights, and operational efficiencies seamlessly come together – remains just that: a promise. The challenge lies in interoperability.
For years, healthcare institutions have grappled with fragmented systems, disparate data formats, and evolving regulatory requirements. The question is no longer whether to integrate but how best to do it. Should healthcare providers build, rent, or buy their data integration solutions? Each approach has advantages and trade-offs, but long-term success depends on choosing a solution that balances control, flexibility, and cost-effectiveness.
Why Interoperability Remains a Challenge
Despite significant advancements in standardisation, interoperability remains a persistent challenge in healthcare. A common saying in the industry – “If you’ve seen one HL7 interface, you’ve seen one HL7 interface” – illustrates the lack of uniformity across systems. Even FHIR, the latest interoperability standard, comes with many extensions and custom implementations, leading to inconsistency.
Henry Adams, Country Manager South Africa, InterSystems
Adding to this complexity, healthcare data must meet strict security, privacy, and compliance requirements. The need for real-time data exchange, analytics, and artificial intelligence (AI) further increases the pressure on organisations to implement robust, scalable, and future-proof integration solutions.
The Build, Rent, or Buy Dilemma
When organisations decide how to approach interoperability, they typically weigh three options:
Building a solution from scratch offers full control but comes with high development costs, lengthy implementation timelines, and ongoing maintenance challenges. Ensuring compliance with HL7, FHIR, and other regulatory standards requires significant resources and expertise.
Renting an integration solution provides quick deployment at a lower initial cost but can lead to vendor lock-in, limited flexibility, and escalating costs as data volumes grow. Additionally, outsourced solutions may not prioritise healthcare-specific requirements, creating potential risks for compliance, security, and scalability.
Buying a purpose-built integration platform strikes a balance between control and flexibility. Solutions like InterSystems Health Connect and InterSystems IRIS for Health offer pre-built interoperability features while allowing organisations to customise and scale their integration as needed.
The Smart Choice: Owning Your Integration Future
To remain agile in an evolving healthcare landscape, organisations must consider the long-term impact of their integration choices. A well-designed interoperability strategy should allow for:
Customisation without complexity – Organisations should be able to tailor their integration capabilities without having to build from the ground up. This ensures they can adapt to new regulatory requirements and technological advancements.
Scalability without skyrocketing costs – A robust data platform should enable growth without the exponential cost increases often associated with rented solutions.
Security and compliance by design – Healthcare providers cannot afford to compromise on data privacy and security. A trusted interoperability partner should offer built-in compliance with international standards.
Some healthcare providers opt for platforms that combine pre-built interoperability with the flexibility to scale and customise as needed. For example, solutions designed to support seamless integration with electronic health records (EHRs), medical devices, and other healthcare systems can offer both operational efficiency and advanced analytics capabilities. The key is selecting an approach that aligns with both current and future needs, ensuring data remains accessible, secure, and actionable.
Preparing for the Future of Healthcare IT
As healthcare systems become more digital, the need for efficient, secure, and adaptable interoperability solutions will only intensify. The right integration strategy can determine whether an organisation thrives or struggles with inefficiencies, rising costs, and regulatory risks.
By choosing an approach that prioritises flexibility, control, and future-readiness, healthcare providers can unlock the full potential of their data – improving patient outcomes, driving operational efficiencies, and enabling innovation at scale.
The question isn’t just whether to build, rent, or buy – but how to create a foundation that ensures long-term success in healthcare interoperability.
Facial pain and discomfort related to the temporomandibular joint (TMJ) is the second-leading musculoskeletal disorder, after chronic back pain, affecting 8% to 12% of Americans. Current treatments for TMJ disorders are not always sufficient, leading researchers to further explore the vast nerve and vessel network connected to this joint – the second largest in the human body.
In a study published in December 2024 in the journal Pain, a research team led by Yu Shin Kim, PhD, associate professor at the The University of Health Science Center at San Antonio (UT Health San Antonio), observed for the first time the simultaneous activity of more than 3000 trigeminal ganglion (TG) neurons, which are cells clustered at the base of the brain that transmit information about sensations to the face, mouth and head.
“With our novel imaging technique and tools, we can see each individual neuron’s activity, pattern and dynamics as well as 3000 neuronal populational ensemble, network pattern and activities in real time while we are giving different stimuli,” said Kim.
When the TMJ is injured or misaligned, it sends out signals to increase inflammation to protect the joint. However, this signaling can lead to long-term inflammation of the joint and other parts of the highly connected nerve network, leading to chronic pain and discomfort. About 80% to 90% of TMJ disorders occur in women, and most cases develop between the ages of 15–50.
Activation at the cellular level
Previous animal studies observed behavioural changes related to pain, but this study was the first to record reactions at the cellular level and their activities. To see which portions of the nerve pathway respond to various types of pain, Kim’s team created different models of pain and observed the neuronal activity with high-resolution confocal imaging, which uses a high-resolution camera and scanning system to observe neurons in action.
The team discovered that during TMJ activation, more than 100 neurons spontaneously fire at the same time. Activation was observed in localised areas of the TMJ innervated to TG neurons. The localisation of this activation highlights the specific neural pathways involved in TMJ pain, offering deeper insight into how pain develops and spreads to nearby areas. The study is also the first to quantify the degree of TG neuronal sensitivity and network activities.
Potential link to migraine, headaches
Chronic TMJ pain in humans is often linked to other pain comorbidity such as migraines and other headaches. Kim’s team observed this crossover in the in vivo model as inflammation of TG neurons spread to the nearby orofacial areas. Kim’s previous research demonstrated how stress-related migraine pain originates from a certain molecule, begins in the dura and innervates throughout the dura and TG neurons. This current study and novel imaging technique further reveals potential connections between the TMJ, migraines and other headaches.
Potential of CGRP treatment
Calcitonin gene-related peptides (CGRP), molecules involved in transmitting pain signals and regulating inflammation, are often found in higher amounts in synovial fluid of TMJ disorder patients. Synovial fluid surrounds joints in the body, helping to reduce friction between bones and cartilage. Higher amounts of CGRP are often associated with increased pain and inflammation. Kim hypothesised in this study that a reduction in CGRP may reduce TMJ disorder symptoms. He found that CGRP antagonist added to the synovial fluid relieved both TMJ pain and hypersensitivity of TG neurons.
Currently, there are no Federal Drug Administration-approved medications for TMJ disorders other than non-steroidal anti-inflammatory drugs (NSAIDS). While some CGRP antagonist medications are FDA-approved for treating migraines, this study suggests these drugs may also provide relief for TMJ disorders. Confirmation of the positive effect of the drug on TMJ pain is a major leap forward in understanding how CGRP affect TMJ pain, said Kim.
“This imaging technique and tool allows us to see pain at its source – down to the activity of individual neurons – offering unprecedented insights into how pain develops and spreads. Our hope is that this approach will not only advance treatments for TMJ disorders but also pave the way for understanding and managing various chronic pain conditions more effectively,” said Kim.
New research out of Michigan State University expands on current understanding of the brain chemical dopamine, finding that it plays a role in reducing the value of memories associated with rewards. The study, published in Communications Biology, opens new avenues for understanding dopamine’s role in the brain.
The research team discovered that dopamine is involved in reshaping memories of past rewarding events – an unexpected function that challenges established theories of dopamine function.
“We discovered that dopamine plays a role in modifying how a reward-related memory is perceived over time,” said Alexander Johnson, associate professor in MSU’s Department of Psychology and lead researcher of the study.
In the study, mice were presented with an auditory cue that had previously been associated with a sweet-tasting food. This led to a retrieval of the memory associated with consuming the food. At this time, mice were made to feel temporarily unwell, similar to how you feel if you’ve eaten something that has upset your stomach.
When the mice had fully recovered, they displayed behaviour as if the sweet-tasting food had made them unwell. This occurred despite the fact that when mice were made to feel unwell, they had only retrieved the memory of the food, not the food itself. This initial finding suggests that devaluing the memory of food is sufficient to disrupt future eating of that food.
The research team next turned their attention to the brain mechanisms that could be controlling this phenomenon. Using an approach by which they could label and reactivate brain cells that were engaged when the food memory was retrieved, the researchers identified that cells producing the chemical dopamine appeared to play a particularly important role. This was confirmed through actions that manipulated and recorded dopamine neuron activity during the exercise.
“Our findings were surprising based on our prior understanding of dopamine’s function. We typically don’t tend to think of dopamine being involved in the level of detailed informational and memory processing that our study showed,” Johnson explained. “It’s a violation of what we expected, revealing that dopamine’s role is more complex than previously thought.”
The team also used computational modelling and were able to capture how dopamine signals would go about playing this role in reshaping reward memories.
“Understanding dopamine’s broader functions in the brain could provide new insights into how we approach conditions like addiction, depression and other neuropsychiatric disorders,” said Johnson. “Since dopamine is implicated in so many aspects of brain function, these insights have wide-ranging implications. In the future, we may be able to use these approaches to reduce the value of problematic memories and, as such, diminish their capacity to control unwanted behaviours.”










{kind=link}