‘Google Earth’ for Human Organs Made Available Online
A new open-access 3D portal that allows users to explore human organs in unprecedented detail, from the whole organ to individual cells, has been launched by an international team led by UCL scientists.
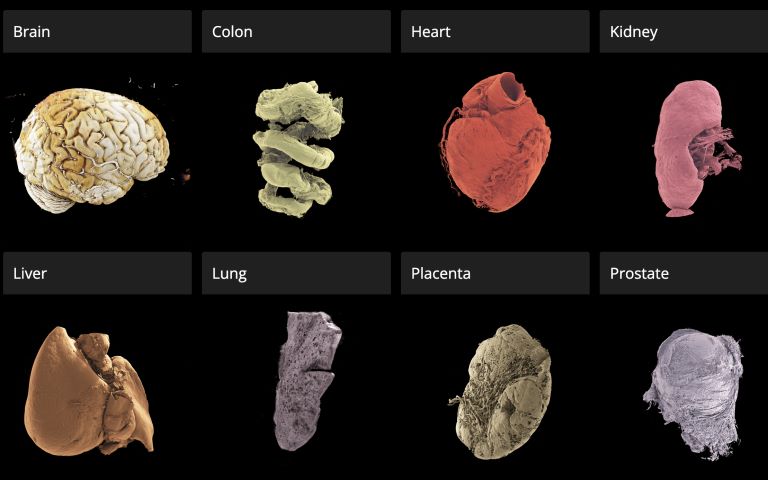
The Human Organ Atlas, described in a new paper in the journal Science Advances, brings together some of the most detailed images of 3D organs ever produced. It enables scientists, doctors, educators, students and the wider public to interactively “fly through” organs such as the brain, heart, lungs, kidney and liver, providing a new way of understanding human anatomy and human diseases.
The resource can be accessed directly through a standard web browser, without specialist software, at this link.
The Atlas is powered by an advanced X-ray imaging method called Hierarchical Phase-Contrast Tomography (HiP-CT), developed at the European Synchrotron (ESRF) in Grenoble, France. HiP-CT uses the ESRF’s Extremely Brilliant Source – a new generation of synchrotron source – which is up to 100 billion times brighter than conventional hospital CT scanners.
This allows researchers to scan entire intact ex vivo human organs (i.e., donated organs) non-destructively and then zoom in to near-cellular resolution (down to less than one micron, 50 times thinner than the size of a human hair).
The technique bridges a century-old gap in medicine between radiology and histology, and represents a major advance in biomedical imaging.
Professor Peter Lee (UCL Department of Mechanical Engineering), principal investigator of the Human Organ Atlas beamtime, said: “To create the Human Organ Atlas, we brought together scientists and medics from nine institutes worldwide. This grouping is continuing to expand, helping gain new insights into diseases from osteoarthritis to heart disease and changing how we learn about the human body.”
Dr Claire Walsh (UCL Department of Mechanical Engineering), Director of the Human Organ Atlas Hub, said: “The Human Organ Atlas shows what team science can achieve at its best – we went into this project wanting this data to be used by others and to help further the understanding of human physiology. The Human Organ Atlas is an incredible resource that will continue to grow. I am personally hugely excited to see how the AI community use the Human Organ Atlas in AI foundation models.”
From Covid-19 to cardiac and gynaecological disorders
Initially developed during the COVID-19 pandemic, the method has already led to high-impact publications and scientific advancements, revealing previously unseen microscopic vascular injury in the lungs of patients who died from Covid-19 or reshaping understanding of cardiac disorders. The technology has also been applied to other organs, providing new insights, for instance, into the way gynecological disorders develop.
Professor Judith Huirne, based at Amsterdam UMC, said: “The virtual 3D histological data derived from Human Organ Atlas hub provides us with valuable insights into the pathogenesis of gynecological disorders. This knowledge is crucial to bridging the current gaps in both understanding and gender disparities.”
This Human Organ Atlas portal is the result of more than five years of collaborative effort between many researchers, engineers, clinicians, and infrastructure specialists, united within the Human Organ Atlas Hub, a consortium involving nine institutes across Europe and the United States.
Since its inception, the team has been committed to open science. Dr Paul Tafforeau, ESRF scientist and pioneer of the imaging technique used to create the Human Organ Atlas, said: “From the beginning, we wanted these data to be accessible to everyone and build an open, shared scientific infrastructure at a global scale. This is a resource for researchers, doctors, educators – but also for anyone curious about how the human body is built.
A unique tool for AI, medicine and education
To the team’s knowledge, this is the highest-resolution open 3D dataset of intact human organs currently available. The Human Organ Atlas currently provides access to: (to be updated)
- 62 organs, 319 full 3D datasets from 29 donors
- 12 organ types, including brain, heart, lung, kidney, liver, colon, eye, spleen, placenta, uterus, prostate and testis
- Multiscale scans, from whole-organ views down to near-cellular resolution (routinely down to 2 µm, as fine as 0.65 microns for some organs)
The portal has been designed to extend far beyond specialist research laboratories. Each dataset can reach hundreds of gigabytes or even over a terabyte in size. The largest one (a brain) is 14 Tb. To make the data usable worldwide, the portal provides:
- Interactive browser-based visualisation (no special software required)
- Downloadable datasets at multiple resolutions
- Tutorials and software tools for analysis
- Regular addition of new data
Beyond advancing anatomical and biomedical research, the atlas is expected to become a major resource for artificial intelligence. Large, high-quality 3D datasets are rare – limiting the development of advanced medical AI systems. The Human Organ Atlas provides a curated, hierarchical dataset ideally suited for training machine-learning models for segmentation, disease detection and super-resolution analysis.
At the same time, it offers powerful new opportunities for medical education and public engagement with science, allowing anyone to explore the human body out of curiosity.
Source: University College London