Weight-related peer teasing is a strong predictor of disordered eating behaviours in adolescents, particularly those at higher genetic risk, new research shows.
Focusing on teenagers, the Flinders University study found that specific environmental factors including peer pressure and conflict with parents can increase the risk of sometimes dangerous disordered eating behaviours – particularly among those with higher genetic risk.
“This study demonstrates that genetic risk for anorexia nervosa exerts a stronger influence on disordered eating behaviours in adolescent girls when combined with adverse parental and peer relationships. These social factors – including parental expectations, criticism, and care, as well as weight-related peer teasing – are pivotal in shaping vulnerability to disordered eating,” says Professor Sarah Cohen-Woods, senior author of the article in the Journal of Child Psychology and Psychiatry.
“It appears that modifiable factors, such as positive peer relationships, and parental behaviour and relationships with their children, may be leveraged to reduce the impact of increased genetic risk for disordered eating behaviours.”
Preventative efforts should target environmental influences such as weight-related peer teasing, and parental interactions and relationships with their children, particularly in those that are genetically at risk.
“For example, high parental expectations or criticism may increase genetic risk for self-induced vomiting and avoidance of eating.
“Weight-related peer teasing was found to increase the influence of genetic factors on disordered eating behaviours, such as objective bulimic episodes.”
The study of 383 Australian teenage twin girls aged between 14 and 19 collected responses to capturing their self-reported experiences of parental expectations, parental criticism, parental care, weight-related peer teasing and parental conflict.
Professor Cohen-Woods, from the Flinders Institute for Mental Health and Wellbeing, says research into the complex interplay between genetic predisposition and environmental factors can in the long term inform and improve clinical and non-clinical solutions to eating disorders.
“The research into anorexia nervosa polygenic risk scores in context with other known environmental risk factors highlights that a person’s genetic risk is not an isolated factor but can be significantly influenced by their social and family environment.”
The research, led by the Blackbird Initiative at the Flinders Institute for Mental Health and Wellbeing, bridges a gap between psychosocial research and molecular genetics, demonstrating a gene-environment interaction using polygenic risk scores and existing parental and peer teasing data.
Researchers, however, say future research is needed with larger cohorts and a broader range of environmental measures to further investigate these complex relationships to guide support and prevention efforts for young people, benefiting everyday families and communities in the future.
The discovery challenges decades of assumptions and points to new hope for patients with depression, Alzheimer’s, and beyond
The most basic assumption about how psychedelic medicine works is at least partially flawed: Psychedelics are altering not just a few specific brain cells, but the vast majority of them, according to a new University of Michigan study.
The research, published in Molecular Psychiatry, shows that even neurons without serotonin 2A receptors – which are important for physiological processes, including mood regulation, perception and cognitive functions – can dramatically benefit from psychedelic compounds. This means that the therapeutic use of psychedelic medicine is far broader than currently appreciated, with important implications for Alzheimer’s disease and PTSD.
“We identified brain regions where most neurons are completely lacking serotonin 2A receptors. Surprisingly, psychedelic treatment was still able to strongly boost connectivity onto these neurons,” said the study’s senior author Omar Ahmed, U-M professor of psychology whose lab studies behavioural neural circuits and attempts to repair them when they go awry in specific disorders.
Psychedelic medicine is being successfully used in clinical trials to treat major depression. For decades it has been presumed that psychedelics work therapeutically by targeting the serotonin 2A receptor found on neurons in the frontal cortex and boosting connections onto those neurons. It has been assumed that frontal neurons with this serotonin 2A receptor were the only neurons benefiting from psychedelic therapy. This is why psychedelic medicine has focused on treating conditions relating to frontal dysfunction, such as major depression, Ahmed said.
When the research team studied the genes expressed in neurons of the entire cortex of the brain, they identified brain regions that did not express the serotonin 2A receptor that is supposed to be needed for psychedelic therapy to work. Ahmed’s lab, including co-first authors Tyler Ekins and Chloe Rybicki-Kler, showed that the retrosplenial cortex, a brain region important for memory, orientation and even imagining oneself in the future, was remarkably devoid of these receptors. The retrosplenial cortex is one of the first brain regions to be impaired in Alzheimer’s disease.
The team then recorded from these neurons lacking serotonin 2A receptors and found that they also show robust neuroplasticity (more synapses) after psychedelic treatment.
“This was a very unexpected finding given the current assumptions about how psychedelic medicine works,” Ahmed said.
The next step used a genetic engineering technique called CRISPR-Cas to reveal the rules that govern this surprising boost in brain connectivity, leading to a revised theory of how psychedelics control the brain’s ability to adapt and change. These new rules do not require neurons to have serotonin 2A receptors themselves to receive a synaptic boost from psychedelics, dramatically increasing the number of brain connections that can be potentially repaired by psychedelic medicine.
“The most successful medicines are those where we fully understand how they work. That is why it is so important to understand the fundamentals of how psychedelic medicine actually works,” Ahmed said.
The new findings are cause for both caution and optimism, he said. Caution, because they show that we need to be wary of psychedelics acting on unintended neurons. Optimism, because they open up the possibility of using psychedelic-like compounds to restore brain connections in Alzheimer’s disease and other disorders involving the retrosplenial cortex, such as PTSD.
“We are actively working on essential preclinical research to test this hypothesis related to Alzheimer’s disease,” Ahmed said.
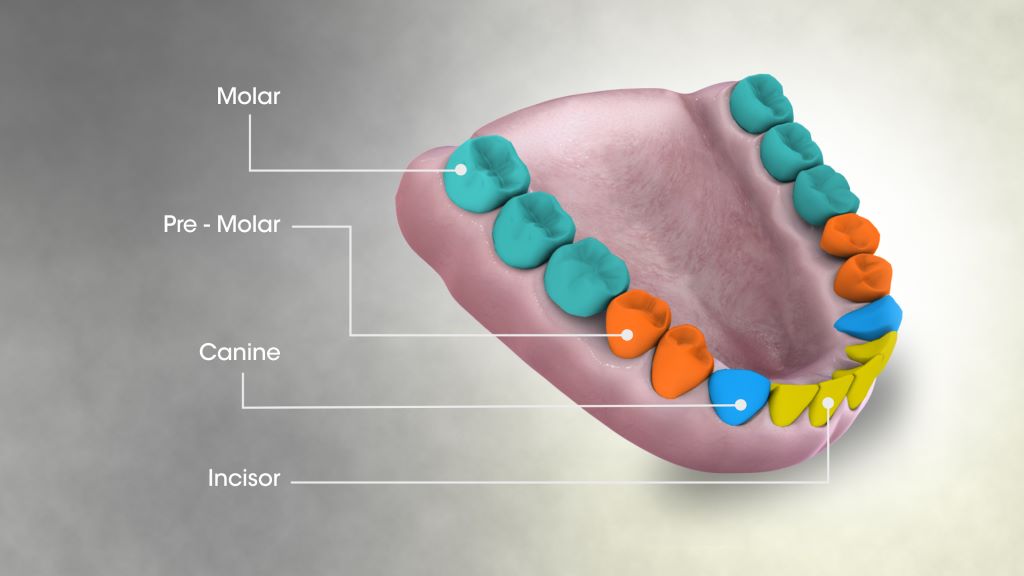
Types of teeth. Credit: Scientific Animation CC4.0
Until now the sensory neurons inside the tooth were primarily thought to send pain signals to the brain, but a new study shows those neurons are multitaskers that also trigger a jaw-opening reflex that almost instantaneously prevents damage and further injury to teeth.
The reflex that pops open the lower jaw was a widely known craniofacial reflex, but until this study the cellular origins of this phenomenon were not known.
University of Michigan researchers in sensory neuroscience, dentistry and mechanical engineering found the origin using special live imaging, behaviour-tracking tools and mice molars to uncover the neurons’ additional role of monitoring the inner tooth and outer enamel.
The discovery and understanding of this additional role shows how important healthy, active nerves are for preserving teeth.
“We suspected there was a more fundamental role for tooth nerves,” said Joshua Emrick, senior author of the study and assistant professor at the U-M School of Dentistry. “When we consider regenerating a tooth pulp, we need to bring back the nerves.”
Emrick’s research team looked at how nerve cells reacted to stimulation of the molar teeth of mice in real time. Their experiments revealed a newly defined, protective role for intradental High-Threshhold Mechanoreceptors, highly specialized sensory neurons that respond to tooth damage. These HTMRs detect dangerous threats and send the message rapidly to the brain for instantaneous action.
“Our study challenges the prior assumption that nerves inside the tooth primarily function to elicit pain and force us straight to the dentist for help,” Emrick said. “If you’ve ever accidentally bitten down on your fork, you’ve probably experienced a startling jolt, but also stopped short of fracturing your teeth. You may thank these intradental HTMRs for that.”
The reflex is really about self-preservation.
“We think protection of the teeth through this jaw-opening reflex is highly conserved among mammals that haven’t developed the ability to replace teeth – like humans or in the molar teeth of mice,” Emrick said. “Our work reports an ability to use these neurons to also elicit pain which will open up possibilities for developing new methods for relieving toothache at the dentist’s office.”
To break it down further, the study, published in Cell Reports, showed that when enamel or dentin is damaged, the neurons fire a response. Follow-up experiments determined what happened after the HTMRs were activated. As previously known, the group identified that they trigger acute pain, but more surprisingly they also witnessed a rapid jaw-opening reflex within 5 to 15 milliseconds of the activation.
While the authors focused their work on understanding how the HTMRs function within the tooth, this important subclass of sensory neurons may protect other oral and body structures from damage. Elizabeth Ronan, postdoctoral fellow at the School of Dentistry and lead author of the work, said the findings are the start of a deeper understanding.
“While we typically think of sensation as giving rise to our perceived external experience of the world, sensory neurons are equally essential in protecting and maintaining our tissues throughout life,” she said. “Much remains to be discovered regarding how sensory neurons function within individual tissues, especially internal ones such as the teeth.”
Dr Deidre McPherson is one of ten women trauma surgeons in South Africa’s public healthcare sector. (Photo: Discovery Foundation)
By Biénne Huisman
Groote Schuur Hospital in Cape Town has one of the busiest emergency centres in the Western Cape. As it turns to the public to raise R20 million for the opening of a new emergency centre, Dr Deidre McPherson chats to Spotlight about the hospital’s trauma frontline.
Deep into the night while most of Cape Town is asleep, trauma surgeon Dr Deidre McPherson slips into work scrubs, hitting the highway to Groote Schuur Hospital to save the lives of critically injured patients.
In a boardroom next to the hospital’s Trauma Centre, McPherson details her solitary early-morning drives along the deserted N1 highway to perform life-saving surgery on people hurt in road accidents, gang violence, and other incidents.
She says she is called out from her home in Bellville past midnight at least once or twice a week. “It’s a surreal feeling,” she says. “I mean driving alone while the rest of the world is sleeping. By now, my husband is used to me leaving at weird times and coming back at like 03:00 or 05:00.”
In South Africa, trauma surgery only became a defined sub-speciality in 2008, meaning a formal training pathway for trauma surgery as its own discipline was created. Trauma surgeons are trained to manage multi-system injuries.
McPerson explains: “We are there at the most crucial moments, when life hangs in the balance. For me, there is nothing more rewarding than seeing a patient arrive critically injured, and walk out the hospital three weeks later, back to their lives.”
R20 million to equip new emergency centre
A new state-of-the-art emergency centre, which includes a new trauma centre, is being constructed at Groote Schuur, beside the existing facility. While it is set to open in 2026, hospital executives are turning to the public for R20 million in additional funding to fit the new premises with upgraded equipment.
As part of the fundraising drive, healthcare professionals recently took journalists on a candid tour of the existing facilities. Inside, corridors are clean but with linoleum floors peeling in places; some patients on trolley beds are stationed against walls, indicating wards filled to capacity.
Just beyond a sign that reads “C14 Welcome to Trauma Centre” – with translations in Afrikaans and isiXhosa – McPherson points out the trauma centre’s resuscitation ward, which can hold six intubated patients, she says. One recent admission can be seen on life support.
Increased capacity and privacy for critically injured patients
McPherson says the new facility will have a more spacious assessment or triage area, where staff decide which patients require immediate life-saving care and which can safely wait.
She says the new trauma centre will expand capacity across all three colour-coded wards. The resuscitation ward (red) will increase from six to ten beds. “This is severe trauma, for example [patients involved in] a motor vehicle accident, with head injury, chest injury and fractures needing life support”. The intermediate ward (yellow) will increase from 12 to 16 beds. “This is moderate trauma, for example, [patients with] multiple fractures, but stable”. The minor ward (green) will increase from 12 to 14 beds. “This is minor trauma for example, [patients with] cuts, bites and bruises – the walking wounded”.
Through the public funding drive, they hope to upgrade the computer system, buy more mobile ventilators for critically injured patients, and get a new full-body X-ray machine for rapid imaging in seconds, which McPherson says is “critical for assessing multiple gunshot or high-impact injuries”.
She says that the centre’s current computer has been in use for over 15 years and frequently stalls. “Sandy, our secretary, is on the phone to IT every second week,” McPherson says, adding that it isn’t necessarily dangerous but that it’s very frustrating. “Time matters so much in trauma,” she emphasises.
In addition, there are lighting issues in some of the examination rooms, with doctors occasionally having to do sutures by headlamp or the flashlight on their phone, McPherson says.
A woman in a male dominated field
During our follow-up interview in the boardroom, McPherson’s gestures are soft, framing her words. Her eyes are level, her cadence precise and unaffected. At present, she is one of ten women trauma surgeons in South Africa’s public sector, compared to 22 men. She is the only woman of four trauma surgeons at Groote Schuur’s trauma centre, which is led by Professor Andrew Nicol.
“Surgery has always been male-dominated and even more so sub-specialties like trauma,” says McPherson. “I was discouraged from following this path by colleagues and even family. This is not a career for women, they said. What if I have a family? The hours are so unpredictable. And there are the violent things we see each day…”
But she was determined. For McPherson, it was a calling, a job she loves. “it doesn’t feel like work,” she says.
Road accidents and gang violence
On average, 1000 patients are admitted to Groote Schuur’s trauma centre per month. Critical injuries, particularly road accidents, spike around Easter, on public holidays, on pay day, and in December, she says. She suggests semigration to Cape Town has seen an additional traffic burden and increased road accidents. Another major contributing factor is accidents involving delivery motorcycle drivers.
In addition, August and September this year have seen a marked month-on-month increase in gunshot wounds, McPherson says, with up to three patients with firearm injuries admitted each day.
“On particularly violent days, that number can rise to as many as 10 patients in 24 hours,” she says.
“What is particularly striking is not just the frequency, but the severity. These are not single gunshot wounds – we often see patients who have sustained multiple injuries, sometimes up to 20 bullet wounds at once.”
This echoes damning murder statistics recently quoted in The Guardian, which notes six people aged from 19 to 25 shot dead over two days in Wallacedene and Eikendal, on the Cape Flats.
Responding, McPherson says: “Sadly what is described in The Guardian is not an isolated incident – it is our daily reality. At Groote Schuur Hospital, we feel that burden first-hand. Every day we are treating teenagers and those in their twenties – who should be building their futures, not fighting for their lives – in our resuscitation bays.”
The latest crime statistics from the South African Police Service lists four precincts on the Cape Flats among the country’s five police stations with the highest murder rates. From January to March this year, Delft had 66 murders, Mfuleni had 65, Nyanga had 63, and Philippi East had 59. This is topped only by Inanda in KwaZulu-Natal which had 74 murders. In each of the last three years over 25 000 people were murdered in South Africa.
This constant cycle of violence is devastating and disheartening, she says, particularly “the high rate of recidivism – when patients return again and again with new injuries”.
For McPherson, cases linked to gender-based violence are especially disturbing. “And yet, as trauma surgeons, we try to focus on what we can do in those critical moments: stop the bleeding, repair the injuries, and give our patients a second chance at life.”
Are there any solutions?
Ultimately, McPherson says the real solution to trauma lies “upstream” in prevention.
“This means tackling the drivers of violence: unemployment, poor housing, failing schools, and the lack of opportunities that trap so many young people in cycles of crime and despair. It also means building safer communities through stronger policing, a justice system that works, and meaningful gun control laws to reduce the number of firearms circulating in our neighbourhoods,” she says.
Then there is preventable road accidents.
“Road traffic injuries remain one of the leading causes of admissions to our unit. As we move into the festive season, I want to urge the public to take responsibility for one another: do not drink and drive, wear seatbelts, and slow down on the roads. These are simple actions that can save lives,” she says.
To this end, she points out the importance of South Africa’s “Arrive Alive” campaign which aims to decrease the number of lives lost on the country’s roads through raising public awareness of road safety. Western Cape officials estimate that 139 people died in road accidents in the province between 1 December 2024 and 11 January 2025, with 627 arrests made for drunk driving.
Childhood inspiration
Born in Bellville to parents who worked in education, the eldest of three sisters, McPherson’s interest in medicine started early, fuelled by a weekly booklet series called How My Body Works. “It was out every Friday, I couldn’t wait for it to arrive. These booklets sparked my fascination with biology and science and it has stayed with me ever since. I still have them at home, packed away in a box,” she says.
McPherson matriculated at Settler’s High School in Parow and studied medicine at Stellenbosch University. She completed her internship at Tygerberg Hospital with a community service year in Atlantis, on the West Coast, where she first saw “how daily violence devastates young people”.
A mother to three-year-old twins, a boy and a girl, McPherson scrolls on her phone to her WhatsApp profile picture, which features her children dressed up in tiny doctor’s scrubs – pink and blue – each with a tiny stethoscope. “It was ‘career day’ so we chose outfits that was easy,” she says, smiling.
McPherson, who also counts a PhD on her resume, says she has processed pangs of “mum guilt” for her children. “My husband has been a constant pillar of support,” she says.
“Plus, I am happy and fulfilled, my children are growing up with a happy mother – but yes, it’s a juggling act, sometimes I have to decide which ball to drop. Is it a rubber ball, that will bounce back, or a glass ball that might shatter?”
To relax, she says she likes to read “sappy romantic fiction” like novels by Danielle Steele.
On her future radar? Becoming a full professor.
In the meantime, McPherson says she believes every encounter is an opportunity to make a difference. “We don’t just treat the injuries, we also try to offer support and counselling, hoping that this time might change the trajectory of a life,” she says.
A new movement in weight management is taking hold in South Africa as the country confronts weight-related illnesses. A powerful class of medication known as GLP-1 therapies is proving highly effective in cutting obesity rates, lowering cancer risk, and improving overall metabolic health. Their growing popularity marks a new frontline in the fight against sugar-driven disease.
A landmark study published in JAMA Oncology has revealed that patients using GLP-1 medications – a class of therapies originally developed for type 2 diabetes – experienced a 17% lower overall risk of cancer.
The data, drawn from over 86 000 patients, showed striking reductions in specific cancers: ovarian cancer risk nearly halved, meningioma cases fell by 31%, and endometrial cancer dropped by 25%.
Dr Tommie Smook, medical practitioner at Dr Smook & Partners (managed by RXME Group), says these findings reinforce the urgent need to fight back against sugar-related disease:
“We are witnessing the medical consequences of unchecked sugar consumption every day in practice. Obesity has become one of the greatest epidemics of our time. If we are serious about safeguarding public health, we must declare a national war on sugar – and GLP-1s are among the most powerful tools we now have to help people reclaim their health.”
What GLP-1s actually do
The body naturally produces GLP-1 – a hormone that regulates blood sugar, appetite, and digestion. GLP-1 medications mimic this process:
• They slow stomach emptying,
• Reduce hunger and cravings,
• Help patients feel satisfied with smaller portions, and
• Stabilise blood sugar levels.
The result is sustained weight loss. Clinical trials consistently show patients losing 10-15% of body weight, particularly when therapy is combined with nutrition, exercise, and professional support. In South Africa, several GLP-1s are now formally registered for obesity and chronic weight management.
But the benefits don’t end at weight loss. International studies have demonstrated improvements in cardiovascular health – lowering blood pressure, reducing inflammation, and decreasing the risk of heart attacks and strokes. Emerging evidence also suggests neuroprotective effects, with potential to reduce risks of dementia and Alzheimer’s disease.
From diabetes treatment to disease prevention
“GLP-1s are no longer just diabetes drugs,” says Dr Smook. “They are transforming the way we think about weight, chronic disease, and prevention. When used responsibly under medical guidance, these therapies can change not only waistlines, but lifespans.”
At Dr Smook & Partners, patients gain access to GLP-1 therapy under the supervision of qualified medical doctors. Medications are prepared only through SAHPRA-approved compounding pharmacies, ensuring quality and safety. This is supported by a multidisciplinary team – dietitians, biokineticists, nurses, and sports physicians, providing holistic care.
Here are the five essentials you should consider before starting GLP-1 therapy:
See a doctor first – these medications require proper screening and monitoring.
Think beyond injections – lifestyle, diet, and exercise remain vital.
Expect an adjustment phase – side effects like nausea are usually temporary.
Protect lean muscle – resistance training and adequate protein intake are essential.
Avoid shortcuts – unregulated, black-market products are unsafe and unpredictable.
A turning point for public health
Obesity is a modern epidemic, and sugar is at the heart of it. GLP-1 medications are not a “quick fix,” but they represent one of the most promising advances in decades – a way to tackle both the causes and consequences of excess weight.
Dr Smook concludes: “The stigma around GLP-1s must end. These therapies are not about vanity – they are about survival. Every patient who regains control of their health is one step closer to breaking sugar’s grip on our society.”