An analysis of data from more than 4.7 million Chinese women showed that those who had low blood sugar levels prior to conception were more likely to have certain adverse pregnancy outcomes – such as their baby being born preterm or with low birth weight. Hanbin Wu of the Chinese University of Hong Kong, in collaboration with the National Research Institute for Family Planning, presents these findings on July 29th in the open-access journal PLOS Medicine.
Prior research has shown that women who are hyperglycaemic before or during pregnancy are more likely to face adverse pregnancy outcomes, as are women who are hypoglycaemic during pregnancy.
However, few studies have explored whether hypoglycaemia detected before pregnancy is associated with adverse pregnancy outcomes for women without pre-existing diabetes. To help clarify, Wu and colleagues retrospectively analysed data on 4 866 919 Chinese women from the National Free Preconception Checkup Project, a free health service for women planning to conceive. Using data from 2013 to 2016, they analysed associations between preconception hypoglycaemia and pregnancy outcomes.
A total of 239 128 of the women had preconception hypoglycaemia. Compared to those with normal preconception blood sugar, they had a higher risk of certain adverse pregnancy outcomes, such as preterm birth, low birth weight, or birth defects. Women with hypoglycaemia tended to be younger than those with normal blood sugar levels and were more likely to have BMIs in the “underweight” category.
However, the adverse pregnancy risks associated with preconception hypoglycaemia varied for women with different BMIs. For instance, underweight women had a higher risk of miscarriage, while overweight women had a lower risk of their baby being large for their gestational age.
On the basis of these findings, the researchers suggest that screening for preconception hypoglycemia could be explored for its potential to improve pregnancy outcomes. Further research could also address some limitations of this study, such as by including women from other countries and more information on patients’ gestational complications.
The authors state, “In addition to paying attention to women with preconception hyperglycemia, our findings call for increased concern for women with hypoglycemia in preconception glycemic screening. These findings emphasize the importance of preconception examination in preventing and managing reproductive health risks for all women planning to conceive, and also highlight the necessity of comprehensive screening and coordinated interventions for abnormal FPG (fasting plasma glucose) prior to and during pregnancy, which is crucial for advancing the intervention window and mitigating the risk of adverse pregnancy outcomes.”
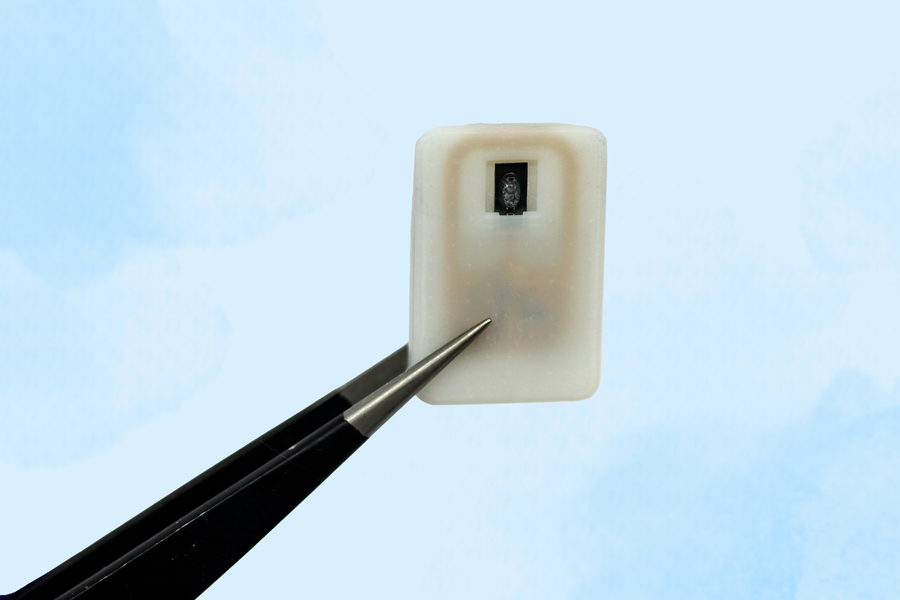
The new implant carries a reservoir of glucagon that can be stored under the skin and deployed during an emergency — with no injections needed.
Caption:A new implantable device carries a reservoir of glucagon that can be stored under the skin and could save diabetes patients from dangerously low blood sugar.
Image: Courtesy of the researchers
For people with Type 1 diabetes, developing hypoglycaemia, or low blood sugar, is an ever-present threat. When glucose levels become extremely low, it creates a life-threatening situation for which the standard treatment of care is injecting a hormone called glucagon.
As an emergency backup, for cases where patients may not realise that their blood sugar is dropping to dangerous levels, MIT engineers have designed an implantable reservoir that can remain under the skin and be triggered to release glucagon when blood sugar levels get too low.
This approach could also help in cases where hypoglycaemia occurs during sleep, or for diabetic children who are unable to administer injections on their own.
“This is a small, emergency-event device that can be placed under the skin, where it is ready to act if the patient’s blood sugar drops too low,” says Daniel Anderson, a professor in MIT’s Department of Chemical Engineering, a member of MIT’s Koch Institute for Integrative Cancer Research and Institute for Medical Engineering and Science (IMES), and the senior author of the study. “Our goal was to build a device that is always ready to protect patients from low blood sugar. We think this can also help relieve the fear of hypoglycaemia that many patients, and their parents, suffer from.”
The researchers showed that this device could also be used to deliver emergency doses of epinephrine, a drug that is used to treat heart attacks and can also prevent severe allergic reactions, including anaphylactic shock.
Siddharth Krishnan, a former MIT research scientist who is now an assistant professor of electrical engineering at Stanford University, is the lead author of the study, which appears today in Nature Biomedical Engineering.
Emergency response
Most patients with type 1 diabetes use daily insulin injections to help their body absorb sugar and prevent their blood sugar levels from getting too high. However, if their blood sugar levels get too low, they develop hypoglycaemia, which can lead to confusion and seizures, and may be fatal if it goes untreated.
To combat hypoglycaemia, some patients carry preloaded syringes of glucagon, a hormone that stimulates the liver to release glucose into the bloodstream. However, it isn’t always easy for people, especially children, to know when they are becoming hypoglycaemic.
“Some patients can sense when they’re getting low blood sugar, and go eat something or give themselves glucagon,” Anderson says. “But some are unaware that they’re hypoglycaemic, and they can just slip into confusion and coma. This is also a problem when patients sleep, as they are reliant on glucose sensor alarms to wake them when sugar drops dangerously low.”
To make it easier to counteract hypoglycaemia, the MIT team set out to design an emergency device that could be triggered either by the person using it, or automatically by a sensor.
The device, which is about the size of a quarter, contains a small drug reservoir made of a 3D-printed polymer. The reservoir is sealed with a special material known as a shape-memory alloy, which can be programmed to change its shape when heated. In this case, the researcher used a nickel-titanium alloy that is programmed to curl from a flat slab into a U-shape when heated to 40 degrees Celsius.
Like many other protein or peptide drugs, glucagon tends to break down quickly, so the liquid form can’t be stored long-term in the body. Instead, the MIT team created a powdered version of the drug, which remains stable for much longer and stays in the reservoir until released.
Each device can carry either one or four doses of glucagon, and it also includes an antenna tuned to respond to a specific frequency in the radiofrequency range. That allows it to be remotely triggered to turn on a small electrical current, which is used to heat the shape-memory alloy. When the temperature reaches the 40-degree threshold, the slab bends into a U shape, releasing the contents of the reservoir.
Because the device can receive wireless signals, it could also be designed so that drug release is triggered by a glucose monitor when the wearer’s blood sugar drops below a certain level.
“One of the key features of this type of digital drug delivery system is that you can have it talk to sensors,” Krishnan says. “In this case, the continuous glucose-monitoring technology that a lot of patients use is something that would be easy for these types of devices to interface with.”
Reversing hypoglycaemia
After implanting the device in diabetic mice, the researchers used it to trigger glucagon release as the animals’ blood sugar levels were dropping. Within less than 10 minutes of activating the drug release, blood sugar levels began to level off, allowing them to remain within the normal range and avert hypoglycaemia.
The researchers also tested the device with a powdered version of epinephrine. They found that within 10 minutes of drug release, epinephrine levels in the bloodstream became elevated and heart rate increased.
In this study, the researchers kept the devices implanted for up to four weeks, but they now plan to see if they can extend that time up to at least a year.
“The idea is you would have enough doses that can provide this therapeutic rescue event over a significant period of time. We don’t know exactly what that is — maybe a year, maybe a few years, and we’re currently working on establishing what the optimal lifetime is. But then after that, it would need to be replaced,” Krishnan says.
Typically, when a medical device is implanted in the body, scar tissue develops around the device, which can interfere with its function. However, in this study, the researchers showed that even after fibrotic tissue formed around the implant, they were able to successfully trigger the drug release.
The researchers are now planning for additional animal studies and hope to begin testing the device in clinical trials within the next three years.
“It’s really exciting to see our team accomplish this, which I hope will someday help diabetic patients and could more broadly provide a new paradigm for delivering any emergency medicine,” says Robert Langer, the David H. Koch Institute Professor at MIT and an author of the paper.
Other authors of the paper include Laura O’Keeffe, Arnab Rudra, Derin Gumustop, Nima Khatib, Claudia Liu, Jiawei Yang, Athena Wang, Matthew Bochenek, Yen-Chun Lu, Suman Bose, and Kaelan Reed.
The research was funded by the Leona M. and Harry B. Helmsley Charitable Trust, the National Institutes of Health, a JDRF postdoctoral fellowship, and the National Institute of Biomedical Imaging and Bioengineering.
Long-term brain damage resulting from neonatal hypoglycaemia can be warded off with proper treatment such as later education and dextrose gel after birth, new studies have found.
The study is the first of its kind to show that stabilising blood sugar levels in neonatal hypoglycaemia prevents brain damage.
Hypoglycaemia is very common, affecting more than one in six babies. Since glucose is the main energy source for the brain and the body, untreated low blood sugar can cause adverse effects on a child’s neurodevelopment up to the age of 4.5 years old.
While hypoglycaemia is known to alter early development, there has been a significant gap in our understanding of how hypoglycaemia can alter a child’s development after early childhood. A study in JAMA investigated the long-term impact on brain development in mid-childhood – ages 9 to 10 – and found that, compared to peers, there was no significant difference in academic outcomes for children exposed to hypoglycaemia as newborns.
“Rich pre-school and school experiences may help a child’s brain to re-organise and improve their academic abilities up to the developmental milestones of their peers,” said Professor Ben Thompson, who is part of the research team.
Following 480 children born at risk of neonatal hypoglycaemia, researchers assessed each child at aged nine to 10 in five key areas: academic achievement, executive function, visual-motor function, psychosocial adaptation, and general health. All child participants were involved in previous studies, providing researchers with information on their neuro-development outcomes at two and 4.5 years old.
This ability to catch-up in neuro-cognitive function could be because of the brain’s plasticity, the researchers suggest.
“It’s a big relief to know that babies who are born with and treated for a condition as common as hypoglycaemia are not likely to suffer long-term brain damage,” Prof Thompson said.
The researchers have also continued studying the efficacy of dextrose gel to treat low blood sugar in the first 48-hours of a newborn’s life, avoiding the need for babies to go to newborn intensive care units immediately after delivery.
In an additional study published in JAMA, the team assessed the later risks of dextrose gel as a treatment for hypoglycaemia in infancy, and found change to the risk of neuro-sensory impairment at age two. This treatment continues to be widely used in a growing number of countries, including Canada, Australia, the United Kingdom and the United States.
A new treatment has been developed that promises a way to prevent potentially lethal hypoglycaemic episodes in children.
For children with Type 1 diabetes, the risk of experiencing a severe hypoglycaemic episode can be quite high. Undetected drops in blood sugar overnight can result in coma and death — an event known as ‘dead in bed syndrome’. As well as being a threat to the child, parents also suffer psychological stress worrying about the situation and often losing sleep.
In severe situations, glucagon injections can stabilise blood glucose levels long enough for parents to get their child medical attention. But in a new study, published in the Journal of the American Chemical Society, Matthew Webber, associate professor of chemical and biomolecular engineering at the University of Notre Dame, is rethinking the traditional use of glucagon as an emergency response by administering it as a preventive measure.
The study describes how Prof Webber and his team successfully developed hydrogels that remain intact in the presence of glucose but slowly destabilise as levels drop, releasing glucagon into the system and raising glucose levels.
“In the field of glucose-responsive materials, the focus has typically been on managing insulin delivery to control spikes in blood sugar,” Prof Webber said. “There are two elements to blood glucose control. You don’t want your blood sugar to be too high and you don’t want it to be too low. We’ve essentially engineered a control cycle using a hydrogel that breaks down when glucose levels drop to release glucagon as needed.”
The water-based gels a three-dimensional structure. Prof Webber describes them as having a mesh-like architecture resembling a pile of spaghetti noodles with glucagon “sprinkled” throughout. In animal models the gels dissolved as glucose levels dropped, releasing their glucagon.
Ideally in future applications, the gels would be administered each night before bed, Webber explained. “If a hypoglycaemic episode arose later on, three or five hours later while the child is sleeping, then the technology would be there ready to deploy the therapeutic, correct the glucose imbalance and prevent a severe episode.”
Since research is in extremely early stages, parents and individuals living with Type 1 diabetes should not expect a therapy available anytime soon, Prof Webber cautioned.
“One of the big challenges was engineering the hydrogel to be stable enough in the presence of glucose and responsive enough in the absence of it,” he said. Another challenge was preventing the glucagon from leaking out of the hydrogel’s mesh-like structure. Though the team was successful in this regard, Prof Webber said he hopes to improve stability and responsiveness with further study.