Dr Jessica Hamuy Blanco, Product and Clinical Risk Executive at Dis-Chem
As the world marks World TB Day on 24 March under the theme “Yes! We can end TB!”, South Africa faces a clear challenge turning awareness into early action.
“TB is all around us,” says Dr Jessica Hamuy Blanco, Product and Clinical Risk Executive at Dis-Chem. “Many people don’t realise that exposure is common. The bacteria can lie dormant for years and only become active when the immune system is compromised.”
Despite widespread awareness, a critical gap remains between what people know about TB and how quickly they act on symptoms. This gap continues to shape outcomes for thousands living with this preventable and curable disease.
According to the World Health Organisation (WHO), approximately 249 000 people in South Africa developed tuberculosis in 2024.
TB remains close to home
Although preventable and curable, TB continues to spread quietly often because symptoms are ignored and treatment is delayed.
“People don’t always recognise the signs early enough or know where to seek help,” says Dr Hamuy Blanco. “This is where informed, trusted healthcare makes the difference.”
South Africa remains one of the countries hardest hit by TB globally. The disease is closely linked to HIV, with weakened immune systems increasing the risk of TB becoming active. At the same time, socio-economic realities such as overcrowding and limited access to healthcare continue to drive transmission.
Delayed diagnosis means individuals remain infectious for longer, placing families and communities at greater risk.
Early detection can change outcomes
Detecting TB early remains one of the most effective ways to reduce its spread and improve recovery. Treatment typically involves a six- to nine-month course of antibiotics, with strong success rates when completed. However early symptoms are often missed.
“The signs can be missed or ignored,” explains Dr Hamuy Blanco. “A persistent cough, fatigue, night sweats or weight loss are easy to dismiss as stress or a lingering illness. That delay gives TB time to spread.”
Creating space for early conversations, whether at a clinic, pharmacy or with a nurse can make the difference between early intervention and prolonged illness.
Finishing treatment is non-negotiable
Another major barrier to ending TB is interrupted treatment. Many patients begin to feel better within weeks and assume they are cured, while others struggle with side effects or the practicalities of repeated clinic visits.
“When treatment is stopped too soon, the bacteria are not fully eliminated,” says Dr Hamuy Blanco. “This is how drug-resistant TB develops, which is far more difficult and costly to treat.”
Supporting patients through the full course of treatment is essential, with clear communication and ongoing support improving adherence.
Bringing care closer to people
“Accessible healthcare is critical in closing the gap between awareness and action”, says Dr Hamuy Blanco. Retail health clinics and digital health platforms are increasingly helping to make care part of people’s everyday lives.
These routine touchpoints create opportunities for people to ask questions, seek advice and act early helping to normalise testing, reduce stigma and support patients throughout their treatment journey.
“Care needs to fit into people’s daily lives,” she adds. “It should be easy to access, easy to understand and supportive from start to finish.”
Turning intent into impact
TB is both preventable and curable, yet it continues to claim lives because of delayed action and incomplete treatment.
“Ending tuberculosis takes more than medicine. It requires a human-centred approach that supports people from early testing through to completed treatment. By breaking down stigma and acting sooner, South Africa can move from awareness to impact,” she concludes.
A major UK-led clinical trial has found that a treatment commonly used to help premature babies breathe offers no benefit for infants on life support with severe bronchiolitis – a seasonal viral illness that hospitalises thousands of babies each year.
Funded by a partnership between the UK’s UKRIMedical Research Council (MRC) and National Institute for Health and Care Research (NIHR), and by Chiesi Farmaceutici SpA, Italy, the Bronchiolitis Endotracheal Surfactant Study (BESS) trial is the largest-ever randomised study of surfactant for bronchiolitis.
Bronchiolitis occurs when a virus – most commonly respiratory syncytial virus (RSV) – infects a baby’s lungs. There is currently no specific treatment for RSV infection, and the illness can be especially severe in premature and newborn infants. Babies with bronchiolitis have reduced levels of surfactant in their lungs, a condition similar to that seen in babies born prematurely. Because surfactant is routinely used to help premature infants breathe more easily, the study team set out to determine whether this therapy could also benefit babies hospitalised with bronchiolitis.
The study ran across 15 children’s hospitals in England, Scotland, and Northern Ireland and involved 232 critically ill babies. However, surfactant did not reduce the time they needed to be on a ventilator (life-support breathing machine).
Professor Calum Semple OBE, the study’s lead from the University of Liverpool and Alder Hey Children’s NHS Foundation Trust, said: “The treatment was safe, but it didn’t make any difference to how long babies stayed on ventilators. We had hoped that surfactant might speed up recovery for these very sick babies, but the evidence doesn’t support this.”
Bronchiolitis is the leading reason why babies are admitted to hospital in the UK during winter. It typically affects babies under one year old and can be especially severe in those born prematurely. While most of the twenty-five thousand babies admitted will recover with oxygen and fluids, around a thousand of the most unwell require intensive care and a ventilator to support their breathing. Currently, there is no other treatment for bronchiolitis, but a vaccine is now being offered to the mother-to-be in the last months of pregnancy.
The BESS trial was designed to give families and clinicians clear answers. It ran over six winter seasons from 2019 to 2024.
Professor Semple added: “While we continue to research better ways to care for these sick babies, I urge Mums-to-be to accept the offer of the RSV vaccine during pregnancy, which will protect their newborn babies from severe bronchiolitis.”
The researchers emphasise that surfactant therapy remains essential for premature newborn babies and advocate for further studies to explore targeted treatments for bronchiolitis.
New TB tests have massive potential for South Africa’s struggle to get to grips with the age-old disease. Making the most of these new tests will require both ambition and smart implementation, argue Gaurang Tanna and Dr Yogan Pillay.
Every day, more than 140 people die from tuberculosis (TB) in South Africa, yet TB is both preventable and curable. Too many people are tested too late, allowing the disease to spread silently through communities and turning a curable illness into a fatal one.
Unlike most other diseases, anyone can contract TB – the bacteria are airborne and just the act of breathing makes us vulnerable to contracting TB. The risk of TB is higher for people with suppressed immunity, malnutrition, or living with cancer or HIV.
Reducing deaths from TB depends on earlier diagnosis, yet many people are diagnosed late, often after prolonged illness, and only once they reach hospitals with advanced disease. There are some opportunities for improvement. Firstly, we need to address persistent weaknesses in where and how TB tests are offered. Secondly, we need to address delays in care seeking, and missed opportunities for testing within health facilities. Finally, we need to close the operational barriers that impede testing. An added challenge that the TB disease presents is that it is often present without any symptoms.
In recent years, South Africa took important steps to strengthen its TB response and intensified efforts to find people with the TB disease through implementation of Targeted Universal TB Testing (TUTT). TUTT is a strategy that promotes systematic testing among high-TB risk groups, like people living with HIV, household contacts of individuals with TB, and people with previous TB, irrespective of symptoms.
South Africa now conducts approximately 3.6 million TB tests annually, representing a 50% increase compared to pre-COVID pandemic testing. However, we need to scale this up considerably if we are to reach the more than six million people living with HIV currently receiving HIV treatment in South Africa as well as all those with TB symptoms who are often missed at facilities.
Despite strong commitments, TB testing in South Africa continues to face several structural constraints.
First, the cost of molecular diagnostics limits the scale of testing. Current molecular TB tests cost approximately R230 per test.
Second, inefficient clinic workflows reduce testing coverage. In busy primary healthcare facilities, this leads to missed TB testing, contributing to prolonged diagnostic delays during which transmission continues and disease severity worsens.
Third, many patients, especially children and people living with HIV, can’t produce sputum, which current tests require, further reducing testing coverage.
Fourth, people with the highest burden of TB, particularly men, often do not attend government clinics. Men account for a disproportionate share of TB in South Africa but remain underrepresented in testing programmes, contributing to delayed diagnoses and ongoing transmission.
Evolving and strengthening testing capabilities in line with the ambitions of the next phase of TB control in South Africa requires leveraging emerging diagnostic tools and redesigning how TB testing is delivered.
New diagnostic tools create new opportunities
Just recently, the World Health Organization updated its recommendations on TB diagnostics, endorsing the use of near-point-of-care tests and use of tongue swabs for people who cannot produce sputum to expand access to TB diagnostics and improve diagnostic efficiency. These new tools provide an opportunity to rethink how testing is organised across the health system.
Tongue swabs offer a promising alternative sample type, enabling testing among patients who cannot produce sputum. It has also been demonstrated to be more acceptable for patients and providers and is easier to collect in clinics.
At the same time, near-point-of-care molecular platforms (such as Pluslife, a test that has been approved by the South Africa’s health products regulatory body) offer the potential to diagnose TB closer to the patient. It substantially reduces costs, to about one-third the cost of current molecular tests, while demonstrating comparable diagnostic performance for TB, making large-scale expansion of TB testing more accessible and affordable. By delivering results rapidly, within an hour, this technology could enable a test and treat approach. TB testing, diagnosis, and treatment initiation could all happen during a single primary healthcare visit. This would reduce the time to start treatment and limit the number of patients lost between diagnosis and treatment.
Clinic workflows need to be redesigned
Patients presenting with TB symptoms often move through multiple stages of the clinic process – registration, triage, waiting areas, and clinician consultations – before TB testing is considered. Improving TB testing requires services redesign for patient convenience and accessibility, and to be much more systematic. A few simple changes could be introduced.
Firstly, introduce a fast-track TB queue, allowing individuals to register digitally and drop off samples without completing a full clinic visit.
Secondly, embed TB symptom screening and sample collection at triage or vital-sign stations. Any patient reporting TB symptoms – cough, fever, night sweats, or weight loss – should have a sample collected while waiting to see a clinician.
Thirdly, for people living with HIV, introduce twin TB testing with annual viral load test (or CD4 for newly diagnosed patients) to systematically test all people living with HIV.
Lastly, we could equip facilities with a near-point-of-care testing platform, like Pluslife, to deliver results before the clinical consultation, allowing TB to be diagnosed rapidly and at lower cost to the health system. It would enable patients to start treatment on the same day.
These approaches could directly address the most persistent diagnostic and linkage gaps in South Africa’s TB programme.
Extending TB testing beyond clinics
New diagnostic platforms also enable TB testing to move beyond government clinics.
A substantial proportion of individuals with TB, particularly men, do not present to clinics and delay seeking care. Near-point-of-care molecular platforms could enable TB testing through alternative delivery channels, including community settings (such as taxi ranks), community pharmacies, workplace clinics, and households through community health worker programmes.
Expanding testing beyond clinics will help identify TB earlier among populations that remain underserved by current services.
From policy ambition to implementation
South Africa’s progress over the past four years demonstrates that intensified testing strategies such as TUTT can help increase TB diagnosis. Sustaining this momentum will require redesigning primary health care services to fully use these emerging diagnostic tools. Three priorities should guide this transition.
First, TB sample collection workflows in clinics should be redesigned to ensure that every symptomatic and at-risk person is tested for TB.
Second, new diagnostic tools should be deployed, including the use of tongue swabs for people who cannot produce sputum, as well as low cost near-point-of-care molecular tests to simplify testing and treatment initiation pathways.
Third, TB testing should be expanded through alternative delivery channels to reach people who do not routinely access government clinic services, especially men, who are less likely to seek care in these settings.
By aligning ambition and new technologies with service redesign, South Africa can significantly reduce diagnostic delays, decrease deaths due to TB and accelerate progress towards TB elimination.
*Tanna is a senior programme officer for TB, and Dr Pillay is the director of HIV and TB delivery at the Gates Foundation.
Disclosure: Spotlight receives funding from the Gates Foundation but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
Note: Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.
Associate Professor Angelique Kany Kany Luabeya speaks about TB vaccine trials and the introduction of TB vaccines in South Africa. (Photo: Supplied)
By Angelique Kany Kany Luabeya
The only tuberculosis vaccine we have is a century old and offers only limited efficacy in children. With leading South African researchers involved in the pivotal clinical trials of three new tuberculosis vaccine candidates, we are on the verge of a major breakthrough, writes Associate Professor Angelique Kany Kany Luabeya.
My uncle died of abdominal TB a few days ago, after facing repeated challenges in getting an accurate diagnosis. For him, the treatment started much too late. To many in his community, my uncle was a respected teacher, a breadwinner, a pillar of support and strength.
In 2026, why are people still dying from a preventable disease that continues to cause unnecessary deaths and hardship?
Why we urgently need a new TB vaccine should be obvious. For the millions who are sick, and for families living with the catastrophic loss of a loved one, the need is painfully clear.
Prior to the emergence of the SARS-CoV-2 virus, TB was the world’s deadliest infectious disease, killing more than 1.5 million people every year. While COVID-19 has since shown an epidemic downturn, TB’s toll remains devastatingly high.
Globally, an estimated 2 billion people are infected with the Mycobacterium tuberculosis that causes TB in humans. In this state, also known as latent TB infection, they do not have TB symptoms and are non-infectious, but the bacteria remain dormant in their bodies. Of these people, about 5 to 10% will go on to develop active TB when their immune system is no longer able to contain the bacteria. This means that they now have TB disease, sometimes without noticeable symptoms, and risks passing it to others. This could be a family member, a friend, or a stranger who happens to be nearby.
TB bacteria have coexisted with humans for millions of years. There is a cure, but treatment alone is not enough to stop transmission. TB mostly affects countries with limited resources because patients struggle to access care or are unable to complete treatment due to side effects or a lack of food to support the rigorous regimen of drugs they must take to cure them. In addition, the rise of multidrug-resistant tuberculosis is now fueling a global health crisis.
In South Africa, recent data from the World Health Organization’s (WHO) Global TB Report indicate progress, with a 57% reduction in new TB cases since 2015. However, TB mortality is still high and is concentrated mainly in poor and vulnerable communities. According to the WHO, TB still claims over 50 000 lives in South Africa every year. The burden is also unevenly distributed, with some geographic areas affected more than others.
A vaccine which prevents TB
Our hopes are now pinned on developing an efficacious vaccine which prevents people from developing TB disease. WHO modelling suggests that a vaccine which prevents most people with latent TB infection from progressing to active disease would have the most rapid impact on the epidemic in high‑burden countries.
The most urgent priorities for protection would be people living with HIV, healthcare workers at risk of workplace exposure, adolescents and young adults who are driving transmission, as well as those with comorbidities such as diabetes that increase their risk of TB diseases and negatively affect treatment outcomes.
The COVID-19 pandemic proved that when human survival is threatened, the scientific community can respond with breathtaking speed, developing multiple effective vaccines in under a year. Sadly, the urgency and resources allocated to finding an effective TB vaccine do not match the scale of its devastation.
For more than a century (since 1921), we have had only one licensed TB jab, which is the bacillus Calmette-Guérin (BCG) vaccine that is given at birth. Despite its limitations in preventing TB that infects the lungs – the main route of transmission – BCG remains a critical tool because it protects millions of babies from more serious forms of TB that can spread through the blood to the brain. But, clearly, the BCG vaccine is not enough.
Hope is on the horizon though, with several novel TB vaccines now in late-stage clinical trials. New vaccines or drugs are evaluated clinically in humans in steps, or phases, for safety, immunogenicity, and efficacy.
The most advanced is M72/AS01E (M72 for short), which is an adjuvanted subunit vaccine under development by the Gates Medical Research Institute and GlaxoSmithKline. In a phase 2 trial, this vaccine showed close to 50% efficacy in preventing TB disease in TB-infected people—the first time a vaccine has achieved this level of efficacy. A pivotal phase 3 trial of this vaccine has now completed enrolment of 20 000 volunteers, including 13 000 people in South Africa, with results expected in 2028. Developers typically apply for registration with regulatory authorities after successful phase 3 trials – so this study is the last big hurdle for this vaccine.
Another promising candidate is the MTBVAC vaccine, a live, whole, attenuated Mycobacterium tuberculosis vaccine developed by Biofabri, in partnership with the University of Zaragoza and sponsored by the International AIDS Vaccine Initiative. It is in a multi-country phase 2b trial in adults and adolescents and a phase 3 trial in newborns, including in South Africa.
BioNTech’s mRNA TB vaccine is also being evaluated in a phase 2a study in South Africa. Funded by BioNTech, this vaccine candidate harnesses mRNA technology, which has proved successful in the COVID-19 response.
Paving the way for acceptance and use
South African researchers are at the forefront of these TB vaccine efforts. Our strengths lie in our robust clinical trial capacity, world-class institutions, commitment to equitable solutions, and regulatory expertise, all of which help accelerate vaccine licensure. As a global policy leader, South Africa co-chairs the Finance and Access Working Group at the WHO TB Vaccine Accelerator Council, advocating for fair distribution and sustainable financing, and has recently co-hosted a vaccine preparedness workshop to position the country for the emergence of late-stage TB vaccines.
But the most important aspect to consider is the vaccine’s acceptability and uptake by a myriad of population groups at risk of TB. We learned from COVID-19 how misinformation can devastate vaccine uptake, leading to unnecessary morbidity and mortality. Confidence in new TB vaccines must be built to maximise impact. The context may be different—TB is an old, well-known enemy that affects people close to us. By involving South African communities in the early stages of vaccine trials, we can ensure their priorities are part of the development agenda.
While we continue to improve TB diagnosis and treatment, the hunt for an effective vaccine continues. After a century of fighting TB with only one vaccine and several antibiotics, we might be on the verge of a breakthrough that could finally shift the trajectory of this ancient and deadly disease.
*Associate Professor Angelique Kany Kany Luabeya is the clinical investigator on the M72 TB vaccine trials being conducted at the South African Tuberculosis Vaccine Initiative based at the University of Cape Town.
Disclosure: The Gates Medical Research Institute mentioned in this article is a non-profit organisation and subsidiary of the Gates Foundation. Spotlight receives funding from the Gates Foundation but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
Note: Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.
With their innovation of a small but powerful handheld device, researchers at the University of Pretoria (UP) are on course to redefine the tuberculosis (TB) screening process, which could ultimately help to combat the TB pandemic more effectively. TB is one of the deadliest infectious diseases worldwide, claiming more than 1.25 million lives each year, of which about 50 000 deaths occur in South Africa. It is the leading cause of death among people with HIV.
MARTI (mycolate antibody real-time immunoassay) is the name of the handheld device that can provide very high certainty that a person at risk does not have TB. Using just one drop of blood – and no laboratory – it is set to change the way TB is detected. It may even be adapted for use in both human and veterinary healthcare. The diagnostic is fast, accurate, affordable and – the intellectual part of it – proudly South African.
An internal validation trial was recently completed to confirm the accuracy of the test. These trial results show remarkable promise in terms of the specificity, sensitivity and accuracy of the diagnostic test, coming close to the range of targets set by the World Health Organization for the “perfect” test, making MARTI an ideal screening and diagnostic tool. An earlier trial demonstrated great potential in using this test to monitor TB treatment; these results were published in the journal Biomarkers in Medicine.
“Many people aren’t aware that TB doesn’t always sit in the lungs – it can be present in bones, joints and the brain,” says Professor Jan Verschoor, former research leader of UP’s Tuberculosis Research Group in the Department of Biochemistry, Genetics and Microbiology and now an emeritus professor of biochemistry who has been leading this discovery. “The ‘gold standard’ TB test that involves growing cultures from lung sputum can take about six weeks, by which time, many more people could have been infected by the patient or the patient’s health could have deteriorated beyond the prospect of cure. From a simple finger-prick blood sample, the MARTI test gives us a result in 30 minutes. This has profound cost and public health implications in a country like South Africa, where we conduct three to five million TB tests a year.
Tuberculosis bacteria. Credit: CDC
Caused by Mycobacterium tuberculosis, this resilient bacterium has long evaded simple detection methods, particularly in regions where healthcare infrastructure is limited. But now, an unexpected hero has emerged in the war on TB: a molecule in the bacterium’s waxy coat – specifically its mycolic acid (MA) – holds the key. These wax-like substances form a nearly impenetrable barrier, making the bacterium both drug-resistant and difficult to detect.
But while other scientists focused on breaking through this barrier, Prof Verschoor took a different approach: what if the wax itself could be used to detect the disease? He was the first to demonstrate that antibodies to the waxes are reliable indicators of active TB, irrespective of whether someone had been vaccinated or was coinfected with HIV.
A key aspect of the innovation came from Carl Baumeister, a PhD candidate under Prof Verschoor. He made the leap from slow laboratory-based biosensing to a handheld device that detects anti-MA antibodies accurately and affordably in less than 30 minutes. The result is a test that’s as clever as it is simple and cost-effective.
Detecting these anti-MA antibodies requires sophisticated sensing technology: the surface of a screen-printed carbon electrode is pre-coated with a thin layer of MA. MARTI works by flowing a drop of blood over this electrode. If a patient has TB, the sensor detects these antibodies in the blood sample; if a patient does not have TB, no signal would be generated since there are no anti-MA antibodies in the blood sample.
“The device fits in the palm of your hand and requires only a single drop of blood – no sputum, no needles, no laboratory,” says Carl Baumeister, Head of Operations of the UP spin-off company MARTI TB Diagnostics. “This may become a game-changer to diagnose TB in paediatric and HIV-positive patients, where obtaining sputum samples is often neither feasible nor safe. The same could apply to the 20% of all extra-pulmonary cases.”
“If MARTI says you don’t have TB, you can trust it,” Baumeister says. “That’s a critical trait when trying to rule out cases during an outbreak or in mass screening campaigns, much like what was needed during the COVID-19 pandemic.
Unlike other TB diagnostics, MARTI offers something rare and powerful: near-perfect negative predictive value in typical screening applications.
The internal validation trial across six healthcare facilities in Tshwane was led by Prof Veronica Ueckermann, Head of Infectious Diseases at Steve Biko Academic Hospital and UP’s Faculty of Health Sciences.
“Collecting, transporting, processing and analysing the samples from the various sites within the temperature and time constraints of the validation trial protocol posed a significant logistical challenge – but we succeeded,” says Mosa Molatseli, a senior research scientist who heads up the MARTI laboratory.
Recognising its potential, UP established the start-up company MARTI TB Diagnostics (Pty) Ltd to develop and eventually commercialise MARTI.
“This is designed to ensure that the technology remains in South African hands while attracting investment and serving global needs,” says Gerrie Mostert, interim CEO of the company. “The next steps are to get investors, funding and partner organisations on board, obtain regulatory approval and start manufacturing the kit. Ultimately, MARTI should be rolled out to clinics worldwide.”
Biologics may be more effective with earlier treatment initiation, especially among children with early polysensitisation or multiple early-childhood risk factors, according to the results of a new study published in Annals of the American Thoracic Society. Screening for these risk factors may help inform targeted early initiation of biologics for asthma.
Robust real-world data on the effectiveness of biologic therapies in children with severe asthma remain limited, particularly across different ages and early-life risk profiles. This evidence gap constrains precision in treatment decisions and clinical guidance.
Children with moderate to severe asthma requiring biologic therapy are most affected, especially those initiating biologic treatment at younger ages and those with early indicators of allergic disease or high-risk asthma histories.
Initiating biologic therapy earlier in childhood – particularly in children with significant early-life risk factors and allergic sensitisation – is associated with greater reductions in severe asthma exacerbations in real-world practice.
Findings highlight the importance of treatment timing and patient history when optimizing outcomes with asthma biologics.
Risks of delayed treatment initiation
Delayed initiation of biologic therapy until adolescence or failure to account for early-childhood risk profiles may reduce potential treatment benefit. These findings highlight the risk of suboptimal outcomes when treatment timing or patient selection does not align with underlying disease risk.
Clinicians should prioritise earlier identification and risk-stratified initiation of biologics in children with severe asthma, particularly those with high early-life risk burden, to maximise treatment benefits.
Study findings support development of care pathways that incorporate earlier, risk-stratified biologic initiation. Decision-making algorithms may benefit from integrating age at treatment initiation and early-life risk indicators, such as polysensitisation and high early disease burden, to better identify children most likely to benefit and reduce severe exacerbations.
Future research may also explore the role of clinical artificial intelligence in supporting these approaches. Clinical AI tools could help identify high-risk paediatric patients earlier and guide treatment timing and patient selection by detecting patterns in real-world clinical data, potentially improving precision in biologic therapy use.
In people with chronic obstructive pulmonary disease (COPD), dysfunctional airway mucus is common. Mucus plugging (mucus that accumulates in the lungs and reduces airflow) and chronic bronchitis are both related to dysfunctional airway mucus. Sometimes mucus plugging and chronic bronchitis co-occur, but it is quite common to have one or the other but not both conditions. Given the limited availability of disease-modifying treatments for COPD, understanding the underlying biology of mucus pathology is critical to identifying new therapeutic targets.
In a new study published in the American Journal of Respiratory and Critical Care Medicine, researchers at Boston University Chobanian & Avedisian School of Medicine have found that mucus plugs in the lungs alter the pattern of gene activity in a way that is similar to chronic bronchitis, suggesting that there may be similar underlying causes to both conditions. It is believed these researchers are the first group to study gene activity differences associated with mucus plugging.
“Mucus plugs are quite common in people with COPD and they are associated with diminished quality of life and increased mortality. By identifying how the presence of mucus plugs impacts the biology of the lung we hope to be able to better treat them, or prevent them from forming in the first place,” says corresponding author Marc Lenburg, PhD, professor of medicine at the school.
The researchers studied participants in the Detection of Early Lung Cancer Among Military Personnel (DECAMP) 2 study who were mostly older US military veterans at high risk for lung cancer due to a history of heavy smoking, many of whom had COPD. Computed tomography was performed on them to determine who had mucus plugs and for those that had them, how extensive they were. From that group, a pulmonologist collected cells from their airways and sequenced the RNA from those cells to determine the level of gene activity. The researchers then compared the gene activity from each individual with the extent of mucus plugging to find genes that had increased (or decreased) activity in individuals with more extensive mucus plugging. Once they had this mucus plugging ‘gene signature’, they compared it with gene signatures from other diseases.
According to the researchers, having a better understanding of how mucus plugging impacts the lung and its relationship to chronic bronchitis may give new clues about how mucus dysfunction develops, which could be helpful for developing new therapies to better treat mucus dysfunction. “By uncovering the molecular pathways that drive mucus plugging and chronic bronchitis, we aim to identify biological targets for earlier diagnosis and intervention. Ultimately, we hope these insights will translate into therapies that restore airway health, reduce respiratory symptoms, and improve the quality of life for people living with these chronic lung diseases,” says coauthor Ehab Billatos, MD, an assistant professor of medicine at the school.
One- and three-month regimens both had few adverse reactions and high rates of completion
Tuberculosis bacteria. Credit: CDC
A study comparing one- and three-month antibiotic treatments to prevent active tuberculosis (TB) finds that a high percentage of patients successfully completed both regimens and suffered few adverse side effects. A team led by Richard Chaisson, of the Johns Hopkins School of Medicine, reports these findings February 10th in the open access journal PLOS Medicine.
Following TB exposure, the World Health Organization has traditionally recommended six to nine months of antibiotic treatment to prevent an active infection from developing, but many individuals fail to complete the long course of medication. Studies have shown that shorter regimens lasting one and three months are effective at preventing TB, but the one-month treatment had only been tested in people living with HIV, and the safety of the two regimens had not been compared in a head-to-head trial.
Researchers performed a clinical trial in 500 people residing in Brazil, who were not living with HIV and had been exposed to TB. They randomly assigned participants to take two antibiotics, isoniazid and rifapentine, daily for one month, or weekly for three months. Both the one- and three-month regimens had similarly high rates of completion, at 89.6% and 84.1%, respectively. Adverse reactions were typically mild or moderate, and occurred at comparable rates in both groups. Both regimens were deemed successful and neither proved superior to the other.
Expanding the number of people who receive preventive therapy is essential for reducing TB infections globally, but these efforts have been hampered by several factors, including the length of the treatments. The new findings provide evidence that a one-month course of antibiotics is safe for patients, regardless of HIV status, and will help clinicians, public health programs, and patients to make informed choices about which regimens to use. Experts hope the success of shorter treatments, combined with the availability of newer generic formulations of the medications, which can be taken at home, will facilitate broader use of preventive therapy for TB.
The authors add, “Prevention of tuberculosis in people at the greatest risk is essential for global control of the disease, and shorter preventive treatment regimens will be instrumental in catalyzing uptake in high-burden countries.”
“Tuberculosis preventive treatment regimens have now been shortened from 6-9 months of daily medication to 1 month of daily treatment or 12 once-weekly doses, a transformational advance. Our study shows that both of the ultra-short regimens are well-tolerated and have high rates of completion.”
“The high rates of treatment completion and excellent safety profile of the short-course regimens will help Brazil and other high-burden countries achieve TB control by facilitating widespread uptake of TB preventive treatment,” states coauthor Betina Durovni.
“Preventing TB with short courses of well-tolerated medicines ensures that millions more people around the world can be protected from the devastating consequences of TB disease,” says coauthor Marcelo Cordeiro-Santos.
Discovery could lead to mRNA therapeutic to reduce the risk of cardiac damage
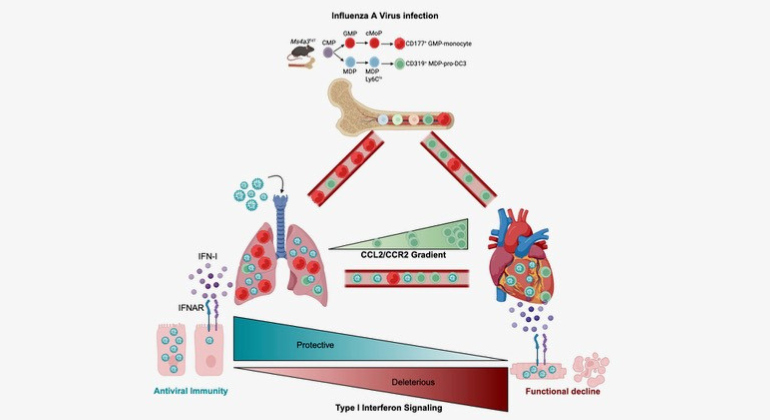
Graphical Abstract summarising the key findings of the paper. The authors found that severe influenza damages the heart by exploiting a specific immune cells and engaging a type-I interferon response. The authors also show that therapeutic silencing of the response mitigates heart damage.
Researchers at Mount Sinai in the US have identified a cellular mechanism linking infections from influenza A viruses (IAVs) to cardiovascular disease, providing critical insights on how influenza can damage the heart and increase the risk of a heart attack or other major cardiovascular event.
Through its work with mouse models and human data, the team also provided evidence that a cutting-edge modified mRNA treatment that dampens an interferon signalling pathway in the heart can significantly mitigate cardiac damage following viral infection while preserving the protective antiviral response of the immune system. The study was published in the February 9 issue of Immunity.
“We have known for years that the frequency of heart attacks increases during flu season, yet outside of clinical intuition, scant evidence exists of the underlying mechanisms of that phenomenon,” says senior author Filip Swirski, PhD, Director of the Cardiovascular Research Institute at the Icahn School of Medicine at Mount Sinai.
“Studies like ours are now shedding valuable light on immune system pathways, like the antiviral cytokine type 1 interferon (IFN-1), that factor into damage to the heart following severe influenza infection. These findings offer great promise for the development of new therapies, which are desperately needed since there are currently no viable clinical options to prevent cardiac damage.”
Influenza A viruses are responsible for an estimated 1 billion infections globally each year, ranging from seasonal flu outbreaks locally to pandemics globally. While most infections are mild and self-resolving, in some cases they can become severe or even fatal, particularly when the virus travels to the heart and triggers the death of cardiomyocytes, specialized muscle cells that are responsible for the rhythmic contraction and relaxation of the heart.
The Mount Sinai team studied autopsies of 35 hospitalised patients who died of influenza and found that more than 85% had at least one significant cardiovascular comorbidity, such as hypertension, and that the majority had multiple comorbidities, including atherosclerosis and cardiac fibrosis, underscoring cardiovascular disease as a major driver of influenza mortality.
The research team also uncovered the mechanism by which cardiac damage occurs. They learned, for example, that a novel subset of white blood cells, known as pro-dendritic cell 3, becomes infected in the lung and, after traveling to the heart, produces large amounts of type 1 interferon. This, instead of fulfilling its mission of clearing the virus from the heart, triggers the death of cardiomyocytes, impairing cardiac output.
“We found that the pro-dendritic cell 3 acts as the ‘Trojan horse’ of the immune system during influenza infection, becoming infected in the lung, trafficking the virus to the heart, and disseminating it to cardiomyocytes. This process causes production of the damaging type 1 interferon that comes with considerable collateral damage to the heart,” explains Jeffrey Downey, PhD, a member of Dr Swirski’s laboratory who served as lead author of the study. “The hopeful news for patients is that by injecting a novel mod-RNA therapeutic that modulates the IFN-1 signaling pathway, we reduced levels of cardiac damage, as evidenced by lower troponin, and improved cardiac function, as measured by higher left ventricular ejection fraction.”
As part of its ongoing research, Dr Swirski’s team is collaborating with Lior Zangi, PhD, Associate Professor of Medicine (Cardiology), and Genetics and Genomic Sciences, at the Icahn school of Medicine at Mount Sinai, to investigate the use of a safe and effective systemic delivery method of the mod-RNA therapeutic to the heart’s muscle cells, instead of the direct injection method used in its proof-of-concept study. Additional work is focused on the pro-dendritic cell 3 itself: why is it so susceptible to influenza and how could its protective capacity be fully harnessed to potentially minimize heart damage exacerbated by cardiovascular disease?
“Pathogens are constantly emerging and evolving, which means our strategies to combat them must evolve as well,” says Dr Swirski. “Better understanding of influenza pathogenesis and immune pathways that are activated throughout the body will help fuel the next stage of advanced care.”
A new test shows promising results for detecting latent tuberculosis infection in resource-limited settings. This is according to a study from Karolinska Institutet, published in the journal Clinical Infectious Diseases.
“This test can help more people with latent tuberculosis to be detected and receive preventive treatment, especially in rural areas in countries with limited resources,” says last author Lina Davies Forsman, a researcher at the Department of Medicine, Solna, Karolinska Institutet.
Tuberculosis remains one of the world’s deadliest infectious diseases. To reduce the number of new cases, infected individuals with latent infection must be detected and offered preventive treatment to avoid active tuberculosis, which can spread the disease to others.
Currently, latent tuberculosis is often diagnosed using a laboratory test called QuantiFERON-TB Gold Plus. This test involves several steps and can take one to two days before the results are available, as well as requiring advanced laboratory infrastructure and trained personnel. This makes it difficult to carry out tests in areas with a high prevalence of tuberculosis where access to laboratories and trained personnel is limited.
Results within 15 minutes
In the new study, researchers from Karolinska Institutet, together with colleagues in Vietnam, have therefore compared this test with another test, TB-Feron. This is a point-of-care test that provides results within 15 minutes and does not require an advanced laboratory or trained personnel.
The study included 345 adult participants in Hanoi, Vietnam, divided into three groups: people with confirmed tuberculosis, people in the same household as people with infectious tuberculosis, and people with no known exposure to tuberculosis. All were tested with both TB-Feron and the established laboratory test QuantiFERON-TB Gold Plus.
The results show that TB-Feron has high sensitivity – 88 percent of individuals with expected positive results were correctly identified. The corresponding figure for QuantiFERON-TB Gold Plus was 92 percent.
However, the specificity, i.e. TB-Feron’s ability to rule out tuberculosis infection in healthy individuals, was moderate at 70 percent. The corresponding figure for QuantiFERON-TB Gold Plus was 96 percent.
Among household contacts, the concordance between TB-Feron and the established test was good, with 92 percent concordance for positive samples.
“It is promising that TB-Feron works so well in an environment with a high disease burden. The test is patient-friendly and easy to use, with rapid same-day results, making it useful in primary care,” says Han Thi Nguyen, pulmonologist and doctoral student at the same department and first author of the study.
The researchers also investigated the reliability of TB-Feron by comparing results from two different groups with laboratory staff. No systematic differences were observed, indicating good reproducibility.