Eating animal-sourced protein foods is not linked to a higher risk of death and may even offer protective benefits against cancer-related mortality, new research finds.
The study, published in Applied Physiology, Nutrition, and Metabolism, analysed data from nearly 16 000 adults aged 19 and older using the National Health and Nutrition Examination Survey (NHAMES III).
Researchers examined how much animal and plant protein people typically consume and whether those patterns were associated with their risk of dying from heart disease, cancer or any cause.
They found no increased risk of death associated with higher intake of animal protein. In fact, the data showed a modest but significant reduction in cancer-related mortality among those who ate more animal protein.
“There’s a lot of confusion around protein – how much to eat, what kind and what it means for long-term health. This study adds clarity, which is important for anyone trying to make informed, evidence-based decisions about what they eat,” explains Stuart Phillips, Professor and Chair of the Department of Kinesiology at McMaster University, who supervised the research.
To ensure reliable results, the team employed advanced statistical methods, including the National Cancer Institute (NCI) method and multivariate Markov Chain Monte Carlo (MCMC) modelling, to estimate long-term dietary intake and minimize measurement error.
“It was imperative that our analysis used the most rigorous, gold standard methods to assess usual intake and mortality risk. These methods allowed us to account for fluctuations in daily protein intake and provide a more accurate picture of long-term eating habits,” says Phillips.
The researchers found no associations between total protein, animal protein or plant protein and risk of death from any cause, cardiovascular disease, or cancer. When both plant and animal protein were included in the analysis, the results remained consistent, suggesting that plant protein has a minimal impact on cancer mortality, while animal protein may offer a small protective effect.
Observational studies like this one cannot prove cause and effect; however, they are valuable for identifying patterns and associations in large populations. Combined with decades of clinical trial evidence, the findings support the inclusion of animal proteins as part of a healthy dietary pattern.
“When both observational data like this and clinical research are considered, it’s clear both animal and plant protein foods promote health and longevity,” says lead researcher Yanni Papanikolaou, MPH, president, Nutritional Strategies.
This research was funded by the National Cattlemen’s Beef Association (NCBA), a contractor to the Beef Checkoff. NCBA was not involved in the study design, data collection and analysis or publication of the findings.
An increase in high-fat, high-fructose foods in people’s diets has contributed to a dramatic increase in type 2 diabetes. This, in turn, has led to an increase in peripheral neuropathy. About half of people with type 2 diabetes are affected, and of these, about half experience severe neuropathic pain.
The damage begins as axons from sensory neurons begin to retract and disappear from the tissues they innervate. New research from the lab of Clifford Woolf, MB, BCh, PhD, director of the F.M. Kirby Neurobiology Center at Boston Children’s Hospital, reveals that months before the damage occurs, immune cells flood into peripheral nerves in an apparent attempt to protect them. This surprising insight, published in Nature, could lead to strategies to prevent peripheral neuropathy or at least minimize and slow the onset of the damage.
Immune cells prevent nerve damage
A team led by Sara Hakim, PhD, a graduate student in the lab, created a mouse model of diabetes induced by a high-fat, high-fructose diet. The model showed that these mice developed all the major features of diabetes within eight to 12 weeks of starting the diet. At about six months, axons in the skin began to degenerate, indicating the presence of neuropathy.
“Diabetic neuropathy takes years, or even decades to develop in humans,” says Hakim, who is now at Vertex. “By using a mouse model in which symptoms slowly develop over months, we were able to catch the progression of the disease over time, and observe those early protective responses when the body is still trying to fight the disease.”
The researchers suspected that peripheral neuropathy is caused by the immune system, so used single-cell sequencing to detect changes in immune cells near sensory neuron axons in peripheral nerves.
One type of immune cell residing in nerves, a pro-inflammatory macrophage, began producing chemokines. These signaling molecules recruited a second population of circulating macrophages, which began infiltrating the nerve 12 weeks after the mice began the diet – as sensory symptoms were starting to appear but before nerve degeneration was seen.
Previously, macrophages were thought to have a pathogenic role in diabetes and were mainly reacting to axon loss. But Hakim, Woolf, and colleagues observed just the opposite.
“To our great surprise, when we blocked infiltration of macrophages into the nerve, neuropathy started getting worse, not better,” says Woolf. “The macrophages were protective. They slowed down the onset of neuropathy and reduced its impact.”
Potential strategies for peripheral neuropathy
The Woolf Lab is now exploring how the infiltrating macrophages protect against peripheral neuropathy. The next step would be to find a way to induce and sustain this protection and identify biomarkers that would flag those people with diabetes who are at risk.
One potential protective strategy might involve accelerating the recruitment of macrophages into nerves; another might involve mimicking their protective function by harnessing compounds they secrete, such as galectin 3.
“Since we could profile the cells and identify what genes they are expressing, we found a number of signalling molecules known to be protective,” says Woolf. “We can now go through that list and check to see which are most active.”
The latest work reinforces the idea that pain isn’t just a disease of neurons, but results from interactions between the nervous system and the immune system. In a study last year, the Woolf Lab discovered thousands of molecular interactions between pain-sensing neurons and different types of immune cells.
Now, the plot is thickening with this example of immune cells acting to prevent painful nerve damage. “We’ve now revealed a novel, slower protective effect of the immune system,” Woolf says.
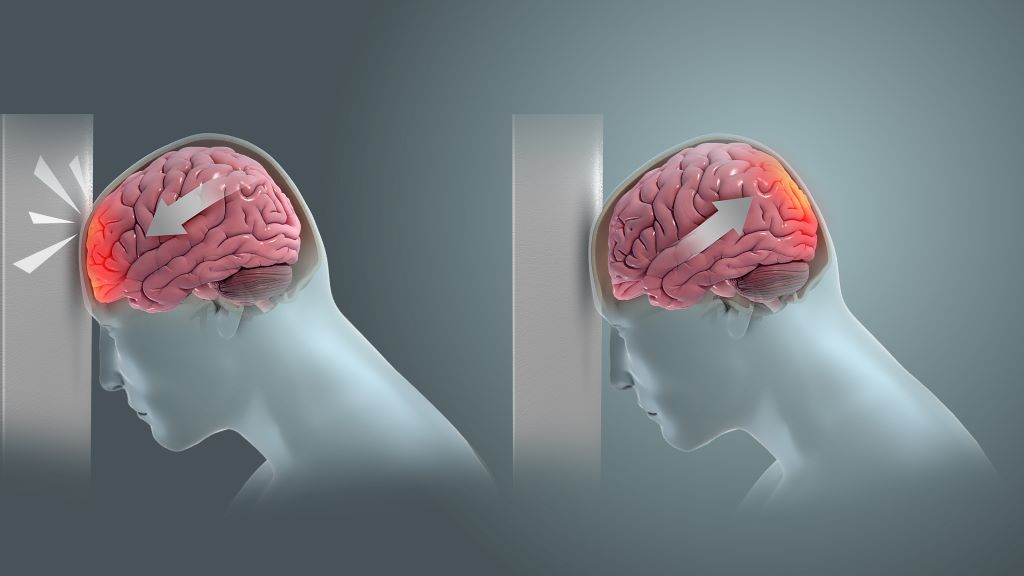
Coup and contrecoup brain injury. Credit: Scientific Animations CC4.0
New research led by investigators at Mass General Brigham suggests a link between a history of traumatic brain injury (TBI) and risk of developing a malignant brain tumour. By evaluating data from 2000–2024 of more than 75 000 people with a history of mild, moderate or severe TBI, the team found the risk of developing a malignant brain tumour was significantly higher compared to people without a history of TBI. The results were published in JAMA Network Open.
“I see these results as alarming,” said co-senior author and corresponding author Saef Izzy, MD, FNCS, FAAN, a neurologist and head of the Immunology of CNS Injury Program at Brigham and Women’s Hospital, a founding member of the Mass General Brigham healthcare system. “Our work over the past five years has shown that TBI is a chronic condition with lasting effects. Now, evidence of a potential increased risk of malignant brain tumours adds urgency to shift the focus from short-term recovery to lifelong vigilance.
“Alongside our earlier findings linking TBI and cardiovascular disease, this underscores the importance of long-term monitoring for anyone with a history of TBI.”
The team divided the severity of TBI between mild, moderate and severe, with participants suffering from incidents ranging from car accidents to falls. In the two categories of moderate and severe, 0.6% of people (87 out of 14 944) developed brain tumours within 3-to-5 years after the TBI, which was a higher percentage than controls. Mild cases of TBI, such as those caused by concussions, were not associated with an increased risk of tumour. The aim of the study was not to establish a cause-and-effect link between moderate-to-severe TBI and malignant tumours, but rather to explore whether an association exists. Determining causality and understanding the underlying mechanisms will require a dedicated translational study in the future.
A previous study showed veterans of the Iraq and Afghanistan wars who suffered TBI experienced an increased risk of brain tumours, but previous studies on civilian populations showed conflicting results. The collaborative team of researchers used an international disease classifying system known as ICD codes to exclude anyone in the study with a history of brain tumour, benign tumours, and risk factors such as radiation exposure.
Previous neurotrauma studies from Mass General Brigham have looked at patients with a history of TBI and found an association with the emergence of anxiety, depression, and other psychiatric, neurological, and cardiovascular diseases, but the current study focuses on malignant tumour development.
Future imaging studies could draw a connection between the location of the TBI and where tumours developed in the brains of participants. The team would like to further study patients with repeated injuries, such as falls.
“While there is an increased risk of tumour from TBI, the overall risk remains low. Still, brain tumour is a devastating disease and often gets detected in later stages,” said lead author Sandro Marini, MD, a neurologist at Mass General Brigham. “Now, we’ve opened the door to monitor TBI patients more closely.”
Rates of inflammatory bowel disease are rising, and there’s currently no cure. IBD can also be deadly: up to 8% of people with the disease develop blood clots, which can lead to heart attack and stroke. New research has uncovered why blood clotting malfunctions in IBD – and identified drugs that normalise blood clotting in human cells and animal models of IBD.
“We think we can leverage these findings to reduce inflammation and the risk of blood clots,” says senior author Aaron Petrey, PhD, assistant professor of microbiology and immunology at University of Utah Health, associate director of the U’s Molecular Medicine Program. “This could be lifesaving.”
Most research into IBD has focused on immune cells. But blood cells called platelets are another key contributor to IBD symptoms. In healthy people, platelets clump together into clots in response to injuries to stop bleeding, and don’t form clots otherwise. But in patients with IBD, platelets are on a hair trigger, ready to form clots at the slightest provocation.
Surprisingly, platelets from IBD patients weren’t clotting via the normal pathways that trigger clotting, says first author Rebecca Mellema, PhD, pathology postdoc. “It’s completely independent of what we would expect.”
“There’s an innate mechanism by blood vessels to tell platelets to stay quiet and not form a clot yet,” Petrey explains. “Once there’s injury or inflammation, that signal can switch over and tell them to form a clot. That’s the process that’s broken in IBD patients.”
IBD platelets appear to clot more often because they don’t have enough of a key protein called layilin, the researchers found. In healthy people, layilin acts as a molecular brake for clotting: it senses the difference between healthy and injured blood vessels and prevents platelets from clotting as long as blood vessels are intact.
But when the researchers deleted the layilin gene in mice, the brakes came off. Without layilin, platelets were extra sticky, forming clots when they shouldn’t.
The researchers also found that platelets from IBD patients only had about 60% of the layilin protein that they should, leaving them constantly on the verge of clotting.
A promising drug target
Layilin prevents unwanted clotting by tamping down the activity of a clot-triggering molecule called Rac1. In mice without the layilin gene – and in people with IBD – Rac1 is always a little bit too active, which means platelets are too prone to forming clots.
But there’s good news. Drugs that prevent Rac1 activity are already in clinical trials for other conditions, and the researchers’ results suggest that these Rac1 inhibitors could be powerful therapeutics for IBD.
One Rac1 inhibitor reduced excessive clotting in human platelets in a dish. The inhibitor also decreased the level of tissue damage in the gut in a mouse model of IBD.
Promisingly, the drug decreased clotting in platelets from IBD patients even more strongly than it affected healthy cells. “We have shown a hyperactivation pathway in resting IBD patient platelets, but they’re also incredibly sensitive to treatment, moreso than those from a healthy person,” Mellema says.
Normalizing Rac1 activity might not only reduce the risk of heart attack and stroke—it could also help alleviate day-to-day IBD symptoms, the researchers say. Excessive clotting can block blood flow in the gut and make inflammation worse, which means that preventing clotting could reduce inflammation.
Unlike established anti-clotting drugs, the researchers say, Rac1 inhibitors shouldn’t lead to an increased risk of dangerous bleeding, which is a serious concern for IBD patients with chronic inflammation. Blocking Rac1 won’t interfere with other, independent pathways that can trigger platelet clotting, so the cells should still be able to form needed clots in response to injury.
“We’re targeting a pathway that is not pre-activated in healthy people,” Petrey says. “So we can address that step of the pathway, and if there’s a significant injury, the platelets can overcome that inhibition.”
Other groups had been looking into the potential of Rac1 inhibitors to reduce inflammation in IBD. The new work emphasises the potential of these drugs to address multiple symptoms. “Paying more attention to what we can do to address these blood clotting risks could significantly improve patient lives,” Petrey says.
Couple or siblings? New study may explain why we prefer partners who are similar to us. Photo by Daniil Onischenko on Unsplash
It is no secret that people are often drawn to romantic partners who seem similar to themselves. This tendency, called assortative mating, has been established in humans (Horwitz et al., 2023; Luo, 2017) as well as other species. Fish, for example, demonstrate the behaviour frequently (Jiang et al., 2013).
Assortative mating has also recently been in focus on social media with the viral Siblings or Dating game, where people guess whether two individuals who look alike are related or a couple.
The idea is well-founded in academic research. Humans have been observed to select partners with similar physical, personality, and demographic traits (Horwitz et al., 2023), which can impact the genetics of populations – creating subgroups that emphasise the presence of shared traits (Abdellaoui et al., 2015).
But selecting a partner like ourselves may not be solely determined by personal choice. A new study soon to be published in Psychological Science suggests that assortative mating can be explained relatively simply by looking at the inheritance of preferred traits and corresponding preferences for those traits.
Coauthors Kaitlyn Harper and Brendan Zietsch from the University of Queensland describe this scenario simply: If you are tall, you may have inherited tallness from one parent (say, your mother) and the preference for tallness in a romantic partner from your other parent (in this case, your father). The combination of those inherited traits means that you exist in the world as a tall person and are attracted to tall people.
The idea that preference for a particular trait could lead to genetic correlations has been discussed in previous research but is a newer concept for evolutionary psychology, especially in the context of assortative mating.
“The pieces were there, but they hadn’t been connected in this way before,” Harper said. “Agent-based modelling helped us connect the dots – by simulating populations, we could see that assortative mating naturally emerged without the need for additional assumptions or processes.”
She added that this research wouldn’t have been possible without an interdisciplinary mindset.
“The mechanism itself is familiar in evolutionary biology, but it wasn’t thought of as an explanation for assortative mating,” she said. “Making that connection only became possible when we looked across the two disciplines.”
To test this theory, the authors ran an agent-based model where partners are chosen according to heritable traits and preferences over 100 generations. They included models with and without selection pressure on the number of offspring within each generation to assess how the theory stands up under more naturalistic conditions.
They found that even with up to 10 preferences for traits in a partner, clear genetic correlations formed between traits and preferences for those traits, which resulted in the agents choosing partners similar to themselves. Models with selection pressure generated less-stable correlations, which the authors attribute to reduced variance in traits.
“The power of this finding is in its parsimony – it shows that a phenomenon which has puzzled researchers for decades can be understood through an explanation that was hiding in plain sight,” Harper said. “And because the mechanism is so general, it can also apply to assortative mating in animals, where many of the explanations proposed for humans wouldn’t make sense.”
A new study from McGill University finds that a high-salt diet triggers brain inflammation that drives up blood pressure.
The research, led by Masha Prager-Khoutorsky in collaboration with an interdisciplinary team at McGill and the Research Institute of the McGill University Health Centre, suggests the brain may be a missing link in certain forms of hypertension traditionally attributed to the kidneys.
“This is new evidence that high blood pressure can originate in the brain, opening the door for developing treatments that act on the brain,” said Prager-Khoutorsky, associate professor in McGill’s Department of Physiology.
Hypertension affects two-thirds of people over 60 and contributes to 10 million deaths worldwide each year. Often symptomless, the condition increases the risk of heart disease, stroke and other serious health problems.
About one-third of patients don’t respond to standard medications, which primarily target the blood vessels and kidneys based on the long-standing view that hypertension begins there. The study, published in the journal Neuron, suggests the brain may also be a key driver of the condition, particularly in treatment-resistant cases.
How salt disrupts the brain
To mimic human eating patterns, rats were given water containing two per cent salt, comparable to a daily diet high in fast food and items like bacon, instant noodles and processed cheese.
The high-salt diet activated immune cells in a specific brain region, causing inflammation and a surge in the hormone vasopressin, which raises blood pressure. Researchers tracked these changes using cutting-edge brain imaging and lab techniques that only recently became available.
“The brain’s role in hypertension has largely been overlooked, in part because it’s harder to study,” Prager-Khoutorsky said. “But with new techniques, we’re able to see these changes in action.”
The researchers used rats instead of the more commonly studied mice because rats regulate salt and water more like humans. That makes the findings more likely to apply to people, noted Prager-Khoutorsky.
Next, the scientists plan to study whether similar processes are involved in other forms of hypertension.
The brain controls the release of glucose in a wide range of stressful circumstances, including fasting and low blood sugar levels.
However, less attention has been paid to its role in day-to-day situations.
In a study published in Molecular Metabolism, University of Michigan researchers have shown that a specific population of neurons in the hypothalamus help the brain maintain blood glucose levels under routine circumstances.
Over the past five decades, researchers have shown that dysfunction of the nervous system can lead to fluctuations in blood glucose levels, especially in patients with diabetes.
Some of these neurons are in the ventromedial nucleus of the hypothalamus, a region of the brain that controls hunger, fear, temperature regulation and sexual activity.
“Most studies have shown that this region is involved in raising blood sugar during emergencies,” said Alison Affinati, MD, PhD, assistant professor of internal medicine and member of Caswell Diabetes Institute.
“We wanted to understand whether it is also important in controlling blood sugar during day-to-day activities because that’s when diabetes develops.”
The group focused on VMHCckbr neurons, which contain a protein called the cholecystokinin b receptor.
They used mouse models in which these neurons were inactivated.
By monitoring the blood glucose levels, the researchers found that VMHCckbr neurons play an important role in maintaining glucose during normal activities, including the early part of the fasting period between the last meal of the day and waking up in the morning.
“In the first four hours after you go to bed, these neurons ensure that you have enough glucose so that you don’t become hypoglycaemic overnight,” Affinati said.
To do so, the neurons direct the body to burn fat through a process called lipolysis.
The fats are broken down to produce glycerol, which is used to make sugar.
When the group activated the VMHCckbr neurons in mice, the animals had increased glycerol levels in their bodies.
These findings could explain what happens in patients with prediabetes, since they show an increase in lipolysis during the night.
The researchers believe that in these patients, the VMHCckbr neurons could be overactive, contributing to higher blood sugar.
These nerve cells, however, only controlled lipolysis, which raises the possibility that other cells might be controlling glucose levels through different mechanisms.
“Our studies show that the control of glucose is not an on-or-off switch as previously thought,” Affinati said.
“Different populations of neurons work together, and everything gets turned on in an emergency. However, under routine conditions, it allows for subtle changes.”
The team is working to understand how all the neurons in the ventromedial nucleus co-ordinate their functions to regulate sugar levels during different conditions, including fasting, feeding and stress.
They are also interested in understanding how the brain and nervous system together affect the body’s control of sugar, especially in the liver and pancreas.
Ultra-processed foods (UPFs) have become public enemy number one in nutrition debates. From dementia to obesity and an epidemic of “food addiction”, these factory-made products, including crisps, ready meals, fizzy drinks and packaged snacks, are blamed for a wide range of modern health problems. Some experts argue that they’re “specifically formulated and aggressively marketed to maximise consumption and corporate profits”, hijacking our brain’s reward systems to make us eat beyond our needs.
Policymakers have proposed bold interventions: warning labels, marketing restrictions, taxes, even outright bans near schools. But how much of this urgency is based on solid evidence?
My colleagues and I wanted to step back and ask: what actually makes people like a food? And what drives them to overeat – not just enjoy it, but keep eating after hunger has passed? We studied more than 3,000 UK adults and their responses to over 400 everyday foods. What we found challenges the simplistic UPF narrative and offers a more nuanced way forward.
Two ideas often get blurred in nutrition discourse: liking a food and hedonic overeating (eating for pleasure rather than hunger). Liking is about taste. Hedonic overeating is about continuing to eat because the food feels good. They’re related, but not identical. Many people like porridge but rarely binge on it. Chocolate, biscuits and ice cream, on the other hand, top both lists.
We conducted three large online studies where participants rated photos of unbranded food portions for how much they liked them and how likely they were to overeat them. The foods were recognisable items from a typical UK shopping basket: jacket potatoes, apples, noodles, cottage pie, custard creams – more than 400 in total.
We then compared these responses with three things: the foods’ nutritional content (fat, sugar, fibre, energy density), their classification as ultra-processed by the widely used Nova system – a food classification method that groups foods by the extent and purpose of their processing – and how people perceived them (sweet, fatty, processed, healthy and so on).
Perception power
Some findings were expected: people liked foods they ate often, and calorie-dense foods were more likely to lead to overeating.
But the more surprising insight came from the role of beliefs and perceptions. Nutrient content mattered – people rated high-fat, high-carb foods as more enjoyable, and low-fibre, high-calorie foods as more “bingeable”. But what people believed about the food also mattered, a lot.
Perceiving a food as sweet, fatty or highly processed increased the likelihood of overeating, regardless of its actual nutritional content. Foods believed to be bitter or high in fibre had the opposite effect.
In one survey, we could predict 78% of the variation in people’s likelihood of overeating by combining nutrient data (41%) with beliefs about the food and its sensory qualities (another 38%).
In short: how we think about food affects how we eat it, just as much as what’s actually in it.
This brings us to ultra-processed foods. Despite the intense scrutiny, classifying a food as “ultra-processed” added very little to our predictive models.
Once we accounted for nutrient content and food perceptions, the Nova classification explained less than 2% of the variation in liking and just 4% in overeating.
That’s not to say all UPFs are harmless. Many are high in calories, low in fibre and easy to overconsume. But the UPF label is a blunt instrument. It lumps together sugary soft drinks with fortified cereals, protein bars with vegan meat alternatives.
Some of these products may be less healthy, but others can be helpful – especially for older adults with low appetites, people on restricted diets or those seeking convenient nutrition.
The message that all UPFs are bad oversimplifies the issue. People don’t eat based on food labels alone. They eat based on how a food tastes, how it makes them feel and how it fits with their health, social or emotional goals.
Relying on UPF labels to shape policy could backfire. Warning labels might steer people away from foods that are actually beneficial, like wholegrain cereals, or create confusion about what’s genuinely unhealthy.
Instead, we recommend a more informed, personalised approach:
• Boost food literacy: help people understand what makes food satisfying, what drives cravings, and how to recognise their personal cues for overeating.
• Reformulate with intention: design food products that are enjoyable and filling, rather than relying on bland “diet” options or ultra-palatable snacks.
• Address eating motivations: people eat for many reasons beyond hunger – for comfort, connection and pleasure. Supporting alternative habits while maximising enjoyment could reduce dependence on low-quality foods.
It’s not just about processing
Some UPFs do deserve concern. They’re calorie dense, aggressively marketed and often sold in oversized portions. But they’re not a smoking gun.
Labelling entire categories of food as bad based purely on their processing misses the complexity of eating behaviour. What drives us to eat and overeat is complicated but not beyond understanding. We now have the dataand models to unpack those motivations and support people in building healthier, more satisfying diets.
Ultimately, the nutritional and sensory characteristics of food – and how we perceive them – matter more than whether something came out of a packet. If we want to encourage better eating habits, it’s time to stop demonising food groups and start focusing on the psychology behind our choices.
A comprehensive five-year analysis of gap cover claims reveals a healthcare funding crisis that’s rapidly escalating across the South African private healthcare sector. Data from Sirago Underwriting Managers shows that its mega gap claims – those exceeding R50,000 – have exploded by 512% in volume and 437% in value between 2020 and 2024.
The numbers tell a stark story: where 89 mega gap claims totalling R6.2 million were paid in 2020, this figure rocketed to 549 claims worth R34 million in 2024. Perhaps most concerning is that claims exceeding R60 000 are now daily occurrences, with the average large loss gap claim sitting at R63 000 – a far cry from the R6000 to R12 000 averages seen pre-2020.
The Perfect Storm: Medical Scheme Erosion Meets Provider Cost Inflation
This upward trajectory reflects a fundamental shift in South Africa’s healthcare landscape. Medical schemes – constrained by affordability, access, aging membership populations, and where private healthcare already consumes up to 20% of household income – are systematically reducing benefits and transferring more risk onto the member, rather than increasing premiums to match out-of-control healthcare provider cost inflation.
Healthcare provider costs have consistently outpaced inflation by more than double for years, yet unlike pharmaceuticals, there’s no pricing regulation on healthcare provider tariffs. In a country facing a dire shortage of healthcare professionals, specialists are free to charge rates often 500%+ higher than medical scheme reimbursements.
The regulatory framework compounds this issue. The Registrar of Medical Schemes mandates that for Prescribed Minimum Benefit (PMB) conditions, where no Designated Service Provider agreement exists, healthcare providers must be paid in full regardless of the charge – essentially providing a blank check.
Breaking Down Sirago’s Large Loss (Mega) Gap Claims Data (2020-2024)
Five-Year Trend Analysis
2021: 118% increase in claims value paid compared to 2020, driven by COVID-19 impacts and deferred elective surgeries.
2022-2024: Average annual increase of 35% year-on-year in large loss claims volumes.
Highest claims: R200,000+ for ischaemic heart disease conditions in the 50+ age group.
Age Demographics Challenge Assumptions
Contrary to expectations, healthcare crises aren’t limited to older populations:
50-65 years: 31% of claims (average: R65,065)
66-75 years: 27% of claims (average: R64,213)
76+ years: 18% of claims (average: R62,773)
30-49 years: 18% of claims (average: R58,116)
0-29 years: 5% of claims (average: R63,360)
The under-49 age group constitutes 23% of all large loss claims, dispelling notions that major health expenses only affect older demographics, and which highlights the risk transfer challenges faced and imposed by medical schemes.
Claims Distribution
62%: R40,000-R60,000
30%: R61,000-R100,000
6%: R101,000-R150,000
2%: R151,000-R210,000
Leading Conditions Driving Claims
Musculoskeletal Dominance
Over 51% of claims across all age groups involve musculoskeletal conditions, with spinal stenosis leading the charge. Medical schemes often impose strict limits on elective musculoskeletal surgeries due to high costs, particularly for internal prosthetics where co-payments can reach 30% of the hospital account if members don’t subscribe to the scheme-imposed protocols.
Cancer and Circulatory Conditions
Each representing 10% of large loss claims, these conditions reflect both the effect from the delayed diagnosis impact of COVID-19 and the high-cost nature of specialised treatments. Malignant neoplasms of the breast, prostate, and colon lead cancer claims, while acute ischaemic heart disease dominates circulatory conditions.
The Exploitation Factor
Gap insurance is increasingly becoming a target for exploitation. Healthcare providers now routinely ask patients upfront about gap coverage before determining charges, creating a troubling paradox where a R700 monthly gap policy might pay R130,000 for an orthopaedic surgery shortfall, while the medical scheme with an R8,000 monthly premium pays just R30,000. This exploitation threatens the sustainability of gap insurance itself. If current trends continue, gap insurance premiums will inevitably rise, making this crucial protection unaffordable for many South Africans.
The Critical Importance of Gap Cover
Despite these challenges, gap cover remains essential, irrespective of medical scheme option. Most medical schemes have deductibles, co-payments, and reimbursement limits that can leave members significantly out of pocket. The gap between scheme payments and specialist charges can be substantial – often 200% to 500% above scheme tariffs and this isn’t limited to basic hospital cover options. Even comprehensive, top-tier medical scheme benefits leave members facing substantial tariff shortfalls for in-hospital procedures.
The Economics of Healthcare Financial Protection
When you consider the potential financial quantum of a shortfall on your medical scheme benefits, and that a gap cover premium is around R700 per month for a family (2025 Sirago Ultimate Gap), and each family member is covered for up to a maximum of R213 000 per annum, it is clear that Gap Cover is a non-negotiable part of your healthcare financing strategy. A single gap claim of R63k, Sirago’s average large loss claim, would be the equivalent of almost 9 years of premium payments at current premium rates.
Sirago’s mega claims data reveals a private healthcare funding system under severe strain. As medical schemes transfer more financial risk to members through tariff shortfalls, co-payments, and exclusions, gap insurance becomes not just “a-nice-to-have” insurance policy, but essential for financial protection.
However, the sustainability of this model depends on addressing the root causes: unregulated provider pricing, systematic benefit erosion, and the exploitation of gap insurance by unscrupulous providers. Without intervention, South Africa’s healthcare funding crisis will continue to deepen, leaving patients to bear an ever-increasing financial burden.
For consumers, the message is clear: always negotiate pricing for planned surgeries and request formal quotes from all medical role players. In a system where healthcare providers are price makers and medical schemes and gap providers are price-takers, informed patient advocacy becomes crucial for financial survival and your continued access to quality private healthcare.
(Claims statistics drawn from Sirago’s Large Loss Claims Analysis, 2020-2025)
Sirago Underwriting Managers (Pty) Ltd is an Authorised Financial Services Provider (FSP: 4710) underwritten by GENRIC Insurance Company Limited (FSP: 43638). GENRIC is an authorised Financial Services Provider and licensed non-life Insurer and a member of the Old Mutual Group.
Note: The content of this article does not constitute financial advice. Sirago Gap cover is subject to terms and conditions and premiums are reviewed annually. For more information go to www.sirago.co.za (Ts & Cs apply).
Weight-loss interventions, including gastric bypass surgery and drugs that prevent dietary fat absorption, can be invasive or have negative side effects. Now, researchers have developed edible microbeads made from green tea polyphenols, vitamin E and seaweed that, when consumed, bind to fats in the gastrointestinal tract. Preliminary results from tests with rats fed high-fat diets show that this approach to weight loss may be safer and more accessible than surgery or pharmaceuticals.
Yue Wu, a graduate student at Sichuan University, will present her team’s results at the ACS Fall 2025 Digital Meeting, a meeting of the American Chemical Society.
“Losing weight can help some people prevent long-term health issues like diabetes and heart disease,” says Wu. “Our microbeads work directly in the gut to block fat absorption in a noninvasive and gentle way.”
Weight gain is caused by genetic and lifestyle factors, including eating a high-fat diet. A high-fat diet is defined by the U.S. Department of Agriculture as one where 35% or more of a person’s daily calories come from fat, as opposed to protein or carbohydrates. Some pharmaceuticals, such as orlistat, inhibit certain gastric enzymes from breaking down dietary fats, leading to less fat being absorbed by the body. Orlistat is a U.S. Food and Drug Administration (FDA)-approved medication and is effective for weight loss. However, for some people it causes serious side effects, including liver and kidney damage.
So, Wu and her colleagues wanted to target the fat absorption process with their weight-loss intervention but do so without negative side effects. “We want to develop something that works with how people normally eat and live,” says Wu.
To get started, the team created tiny plant-based beads that spontaneously form through a series of chemical bonds between the green tea polyphenols and vitamin E. These structures can form chemical tethers to fat droplets and serve as the fat-binding core of the microbeads. The researchers then coated the spheres in a natural polymer derived from seaweed to protect them from the acidic environment of the stomach. Once ingested, the protective polymer coating expands in response to the acidic pH, and the green tea polyphenols and vitamin E compounds bind to and trap partially digested fats in the intestine.
The microbeads are nearly flavourless, and the researchers foresee them being easily integrated into people’s diets. For example, the microbeads could be made into small tapioca- or boba-sized balls and added to desserts and bubble teas.
The researchers assessed the microbeads as a weight-loss treatment in rats. They put the animals into three groups (eight rats per group), those which were fed a high-fat diet (60% fats) either with or without microbeads and those which were fed a normal diet (10% fats) for 30 days. Rats fed the high-fat diet and microbeads:
Lost 17% of their total body weight, while rats in the other groups didn’t lose weight.
Had reduced adipose tissue and less liver damage compared to rats fed the high-fat and normal diets without microbeads.
Excreted more fat in their feces compared to rats not given microbeads. The extra fat in the rats’ feces had no apparent ill effects on the animals’ health.
Additionally, the eight rats on high-fat diets that consumed microbeads showed similar intestinal fat excretion, but without the gastrointestinal side effects the researchers observed with a fourth group of rats they treated with orlistat.
Wu and her team have started working with a biotechnology company to manufacture the plant-based beads. “All the ingredients are food grade and FDA-approved, and their production can be easily scaled up,” says Yunxiang He, Sichuan University associate professor and co-author on Wu’s presentation.
They’ve also initiated a human clinical trial in collaboration with the West China Hospital of Sichuan University. “This represents a major step toward clinical translation of our polyphenol-based microbeads, following our foundational results,” says Wu. “We have officially enrolled 26 participants in our investigator-initiated trial, and we anticipate that preliminary data may become available within the next year.”