Throwing a little heat on your meal might be an effective strategy for cutting back on calories, according to a new study led by researchers at Penn State.
Scientists at the University’s Sensory Evaluation Center examined how increasing “oral burn” – the spicy taste from ingredients like chili pepper – affects how much food people consume during a meal. The findings, available online now and slated to publish in the October issue of the journalFood Quality and Preference, suggest that making the meal slightly spicier led participants to eat less, consuming fewer calories.
“We know from previous studies that when people slow down, they eat significantly less,” said Paige Cunningham, a postdoctoral researcher and lead author on the study who earned her doctorate in nutritional sciences from Penn State in 2023. “We suspected that making a meal spicier might slow people down. We thought, let’s test, under controlled experimental conditions in the lab, if adding a small amount of spice, but not so much that the meal is inedible, will make people eat slower and therefore eat less.”
The researchers found that increasing spiciness slightly using dried chili pepper slowed down eating and reduced the amount of food and energy consumed at a meal, all without negatively affecting the palatability of the dish.
“This points to added chilies as a potential strategy for reducing the risk of energy overconsumption,” said John Hayes, Penn State professor of food science and corresponding author on the paper. “While portion control wasn’t the explicit goal of this study, our results suggest this might work. Next time you’re looking to eat a little less, try adding a blast of chilies, as it may slow you down and help you eat less.”
Plastic pollution is one of the defining environmental challenges of our time – and some of nature’s tiniest organisms may offer a surprising way out.
In recent years, microbiologists have discovered bacteria capable of breaking down various types of plastic, hinting at a more sustainable path forward.
These “plastic-eating” microbes could one day help shrink the mountains of waste clogging landfills and oceans. But they are not always a perfect fix. In the wrong environment, they could cause serious problems.
Plastics are widely used in hospitals in things such as sutures (especially the dissolving type), wound dressings and implants. So might the bacteria found in hospitals break down and feed on plastic?
Get your news from actual experts, straight to your inbox.Sign up to our daily newsletter to receive all The Conversation UK’s latest coverage of news and research, from politics and business to the arts and sciences.
To find out, we studied the genomes of known hospital pathogens (harmful bacteria) to see if they had the same plastic-degrading enzymes found in some bacteria in the environment.
Pseudomonas bacteria. Source: Wikimedia CCO
We were surprised to find that some hospital germs, such as Pseudomonas aeruginosa, might be able to break down plastic.
P aeruginosa is associated with about 559,000 deaths globally each year. And many of the infections are picked up in hospitals.
Patients on ventilators or with open wounds from surgery or burns are at particular risk of a P aeruginosa infection. As are those who have catheters.
We decided to move forward from our computational search of bacterial databases to test the plastic-eating ability of P aeruginosa in the laboratory.
We focused on one specific strain of this bacterium that had a gene for making a plastic-eating enzyme. It had been isolated from a patient with a wound infection. We discovered that not only could it break down plastic, it could use the plastic as food to grow. This ability comes from an enzyme we named Pap1.
Biofilms
P aeruginosa is considered a high-priority pathogen by the World Health Organization. It can form tough layers called biofilms that protect it from the immune system and antibiotics, which makes it very hard to treat.
Our group has previously shown that when environmental bacteria form biofilms, they can break down plastic faster. So we wondered whether having a plastic-degrading enzyme might help P aeruginosa to be a pathogen. Strikingly, it does. This enzyme made the strain more harmful and helped it build bigger biofilms.
To understand how P aeruginosa was building a bigger biofilm when it was on plastic, we broke the biofilm apart. Then we analysed what the biofilm was made of and found that this pathogen was producing bigger biofilms by including the degraded plastic in this slimy shield – or “matrix”, as it is formally known. P aeruginosa was using the plastic as cement to build a stronger bacterial community.
Pathogens like P aeruginosa can survive for a long time in hospitals, where plastics are everywhere. Could this persistence in hospitals be due to the pathogens’ ability to eat plastics? We think this is a real possibility.
Many medical treatments involve plastics, such as orthopaedic implants, catheters, dental implants and hydrogel pads for treating burns. Our study suggests that a pathogen that can degrade the plastic in these devices could become a serious issue. This can make the treatment fail or make the patient’s condition worse.
Thankfully, scientists are working on solutions, such as adding antimicrobial substances to medical plastics to stop germs from feeding on them. But now that we know that some germs can break down plastic, we’ll need to consider that when choosing materials for future medical use.
A tender for a circumcision device, set to be used in all provincial health care centres and the military, is under legal scrutiny amid claims that the device is untested and unsafe.
Unicirc Pty Ltd has filed papers in the Pretoria High Court seeking to review and set aside the award of the tender to CircumQ RF Pty Ltd amid claims that the CircumQ device is “vastly inferior” compared to its own and others.
In his founding affidavit, Dr Cyril Norman Parker said that the application was “in the public interest” to ensure only safe and proven surgical devices are used in circumcision procedures.
“There is no publicly available information even to suggest that CircumQ’s device is such a device,” he said.
Parker – who has extensive circumcision experience – and his wife, Elizabeth Pillgrab-Parker, co-founded and continue to work in two primary health care centres they established in Mitchells Plain and Sea Point in the Western Cape under the auspices of Simunye Health Care.
Parker says he has worked in the area of male circumcision for 30 years, in particular as an HIV prevention strategy.
They are also the co-directors of Unicirc, which has the licence to distribute and sell a single-use circumcision device for safe and cost effective circumcision. The device “has significant capacity for scaling up circumcision procedures”, Parker said.
Unicirc bid for the tender for the supply of a surgical aid to be used at the nine departments of health and the Department of Defence.
Parker said he and his wife set up the Simunye health care centres when HIV prevalence was high.
“The conclusive results of three landmark clinical trials gave cause for optimism that circumcision could reduce female to male transmission of HIV by between 50 and 60%,” he said.
In terms of a policy decision taken by the National Department of Health, circumcision services were offered to all males aged ten and above.
“Our role, as service providers, is to ensure that we provide that service safety. In so far as ten to 14-year-olds, this means the strict use of device-based methods that avoid the need for sutures which brings complication rates down to less than 1.5%.”
He said he had performed over 3000 circumcisions across all age groups using multiple techniques.
“What is absolutely clear is that in order to provide services to everyone in need, a surgical-only approach has to be abandoned in favour of a device approach. But not all devices are the same.
“We conceptualised the development of a new circumcision device to improve safety, efficiency and accessibility.”
He said the Unicirc device, which is manufactured overseas, allowed for a complete circumcision in one visit, performed by a single health care provider, using a local anaesthetic and without any sutures.
The whole procedure is completed in about ten to 12 minutes and with proper training, it can also be performed by nurses.
“It has now been used for more than ten years by a range of different health care providers. More than 7,500 procedures have been performed in all ages in both public and private health care sectors. No severe adverse events have been reported and excellent cosmetic results have been achieved.
“It has resulted in the doubling of the number of circumcisions that can be performed safely in a day, a significant reduction in complications and increased client satisfaction,” Parker said.
When the World Health Organisation (WHO) published its (device) guidelines in 2020, only the Unicirc device came close to meeting the requirements. The manufacturer had now started the process of securing WHO pre-qualification. (WHO pre-qualified devices have to meet strict standards of quality, safety and efficacy.)
The device had also been tested in medical trials.
In contrast, Parker said, very little was known publicly about the CircumQ device.
“I am not aware of any peer-reviewed publications that consider its use. It has not been reviewed in any of the WHO literature I have perused or in any systematic review of circumcision devices that I have read. This is in contrast to the Unicirc device as well as other products.
“While I have come across two studies, I have not been able to find out anything about this research and I have not seen any evidence to suggest that it is close to being prequalified or even evaluated by WHO.”
Parker said however, he had studied its design, read training material and spoken to various experts and researchers and health care workers who had used that device and later attended training on the Unicirc device.
“It is vastly inferior. Sutures are required, increasing healing time and requiring a follow up visit. It increases patient discomfort and the risk of infection, the procedure takes longer and it’s more difficult to scale up because it requires two operators,” he said.
“But it’s not just a question of which device is better. There is simply no scientific data supporting the use of it.
“In the absence of that, it would be highly irresponsible to recommend its use, especially in the vulnerable ten to 14 age group. It places young boys at unnecessary risk of potentially irreparable harm and undermines the circumcision programme as a whole.”
He said while the tender was awarded in August 2023, “the public health system was far from ready to implement it”.
This was apparent from a letter from National Treasury, dated March 2025, in which it was stated that because of delays in training, service providers were allowed to continue using the conventional dorsal slit surgical method.
Parker submitted that the tender should be reviewed and set aside, and a new bidding process should start afresh.
Unicirc has called on the Treasury to provide a record of its decision-making process after which it may file a further affidavit. This will be provided by 30 May.
So far only the Treasury respondents have filed notices of opposition and they have yet to file affidavits.
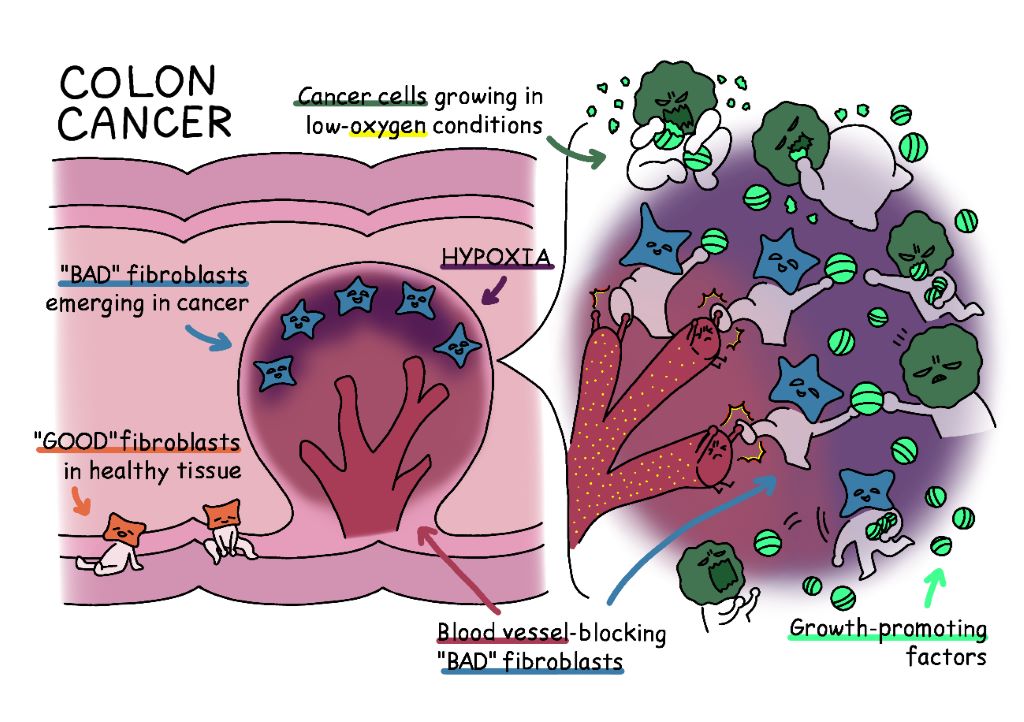
Fig. 1. In healthy colon tissue, “good” fibroblasts help support tissue architecture. However, in colon cancer, these fibroblasts transform into “bad” fibroblasts in low-oxygen areas near the tumour surface. These “bad” fibroblasts block the formation of blood vessels, keeping their surroundings in an oxygen-deprived state, which supports their own survival. At the same time, they release growth-promoting factors that act like supplements for cancer cells. While it may seem unexpected that hypoxia supports tumour growth, this study reveals that localised hypoxic environments can accelerate cancer progression.
To effectively battle cancer, scientists must study the battlefield. Now, in a recent study published in Nature Communications, a multi-institutional research team including The University of Osaka has discovered some crucial intel: localised hypoxia in the colon cancer microenvironment can promote tumour growth.
Until recently hypoxia was thought to suppress tumour progression. Consequently, drugs that block the supply of oxygen to tumours were being used to treat cancers. But these treatments had mixed results; sometimes even accelerating tumour growth. Understanding why this happens has become an urgent question in cancer research.
“We uncovered a surprising mechanism by which hypoxia may promote tumour growth, and it involves the formation of cells called inflammatory fibroblasts,” explains lead author of the study, Akikazu Harada.
The research team found that when oxygen becomes scarce in certain areas of a colon tumour, the surrounding fibroblasts (normally ‘good’ cells that support tissue structure) transform into harmful inflammatory fibroblasts. The altered cells release factors that help tumours grow, such as epiregulin. In addition, they release Wnt5a protein, which helps maintain a low-oxygen state by inhibiting new blood-vessel formation at the site of its release, thereby maintaining hypoxia.
To validate the findings from the mouse model in human samples, the researchers pooled data from human samples obtained from patients with a healthy colon, colon cancer, and those with inflammatory bowel disease. Later, they analysed the data and compared their findings with data from mice.
“We found that the malignant transformation of fibroblasts and the induction of Wnt5a-secreting fibroblasts are commonly observed in both mouse models and human samples,” says Akira Kikuchi, senior author of the study.
This insight into the potential pathology of colon cancer and inflammation can provide the blueprints for a new cancer battle strategy: drug therapies that target Wnt5a-producing fibroblasts. As a result, fibroblasts are now being recognised as a key ‘third’ therapeutic target, complementing traditional treatments targeting cancer cells and immune cells.
This finding holds special importance for colon cancer, which is the leading type of cancer in Japan. Additionally, the observed pathological changes of fibroblasts could also apply to chronic inflammatory disorders like inflammatory bowel disease, offering fresh insights into their mechanisms and potential new treatment strategies for these challenging conditions.
Johannesburg, 26 May 2025: Despite national guidelines and access to essential medicines, severe asthma remains under-recognised and inconsistently managed within South Africa’s healthcare system. It is therefore critical to address ongoing patient challenges, particularly regarding access to diagnostic tools, limited use of phenotyping, and the imperative to align clinical practice with international best practice recommendations.
The Severe Asthma Index 2025 found that South Africa scored below the global average in four out of five domains, revealing persistent gaps in policy coordination, equitable access, diagnostic capacity, and environmental health.¹ᵃ Of concern is the continued reliance on oral corticosteroids (OCS) without proper assessment or referral, especially where evidence-based, targeted biologics remain inaccessible or unfunded.1b+2a
Understanding asthma in South Africa
South Africa has robust asthma guidelines, but the absence of a national asthma strategy and lack of participation in global severe asthma registries limit insight into outcomes and weaken care coordination. Specialist care and phenotyping are largely confined to urban centres, and national data on hospitalisations and treatment outcomes is scarce. Although reported asthma-related societal costs and disability adjusted life years (DALYs) are relatively low, this likely masks the true burden among patients with severe, underdiagnosed, or poorly controlled disease.¹ᵇ Traditionally, asthma mortality in Southern Africa has been considered as relatively high due in large part to short-acting beta-agonists (SABAs) overuse.3
Environmental factors compound these challenges. High levels of particulate matter (PM2.5) and poor indoor air quality contribute significantly to disease severity, particularly in low-income areas. Meanwhile, access to advanced diagnostics and therapies remains limited. Biologic add-on therapies and fractional exhaled nitric oxide (FeNO) testing are not routinely available in the public sector, leaving most patients dependent on standard treatments with few options for escalation if the disease remains uncontrolled.¹ᵇ
Rethinking corticosteroid use
The Severe Asthma Index 2025 highlights the widespread use of oral corticosteroids (OCS) in South Africa as a persistent pattern that may pose long-term health risks if not carefully managed or replaced by more targeted therapies. While OCS play a critical role in treating acute exacerbations, frequent or prolonged use is linked to serious side effects, including osteoporosis, adrenal suppression, diabetes, and infections.²ᶜ
“There’s growing awareness that long-term OCS use can lead to significant health risks,” says Dwayne Koot, Medical Manager at Sanofi South Africa. “For severe asthma, the shift is towards biologic therapies that specifically target the underlying inflammation, not just the symptoms.1c As a simple regimen (where available), inhaled corticosteroid–formoterol combinations are now recommended as the preferred reliever across all severity levels.3 If high-dose ICS-LABA is needed, its use should be limited to 3 – 6 months, prompting phenotyping and biologic therapy add-on if asthma is not controlled. Low-dose maintenance OCS should only be considered as a last resort if no other options are available.”
Improving diagnosis and referral
Access to diagnostic tools remains uneven across South Africa, particularly in the public sector. Spirometry is not routinely available at primary care level, while FeNO testing, oscillometry, and biomarker analysis are largely limited to research centres or private practices.¹ᵇ
“This makes it difficult to accurately diagnose, phenotype, and manage asthma, potentially leading to suboptimal treatment decisions and poorer patient outcomes,” says Koot.
“There’s an opportunity to enhance the referral pathway to specialists and expand access to advanced diagnostic tools by defining referral criteria and partnering with specialised centres,” Koot says. “Routine phenotyping at GINA step 5, crucial for tailoring treatment plans and identifying suitable candidates for biologic therapies, is currently limited in many healthcare settings. Expanding these capabilities would enable a more personalised approach to asthma management.”3
To help close these gaps, the Severe Asthma Index 2025 recommends piloting basic phenotyping tools such as eosinophil counts at regional hospitals, establishing asthma registries to monitor outcomes and access, and expanding clinician training in severe asthma diagnosis and escalation pathways.¹ᵇ “Better data and better training could transform how we identify and treat severe asthma,” says Koot.
Next steps for clinical practice
Healthcare professionals have a pivotal role to play in strengthening asthma care — from recognising poor control early to ensuring patients access the most appropriate treatment in a timely manner. This includes reassessing those with persistent symptoms, reinforcing correct inhaler technique, referring for further investigation when needed, and considering alternative therapies when conventional options are no longer sufficient.3
South Africa already has many of the essential components in place: national treatment guidelines, access to key medicines, and clinical expertise. The next step is to ensure that patients with severe asthma are consistently identified, supported, and offered the full range of available interventions.
“As the World Asthma Day 2025 theme reminds us, the goal is to ‘Make Inhaled Treatments Accessible for ALL’, because inhaled medications are vital not just for preventing attacks, but for controlling chronic inflammation,” says Koot. “We encourage healthcare practitioners and policy makers to help make appropriate, evidence-based asthma care a reality for every South African asthmatic .”
For more information about asthma management and Sanofi’s commitment to respiratory health, please visit www.sanofi.co.za